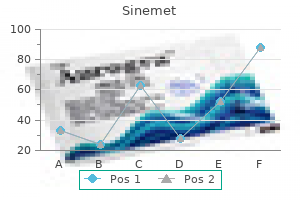
Discount sinemet 300 mg with visa
Management Unstable sufferers or sufferers with active hemorrhage are managed surgically 97110 treatment code 110 mg sinemet buy mastercard. Left lateral portal vein enlargement medications zetia cheap 110 mg sinemet fast delivery, arterial section hyperenhancement, and venous phase washout (arrow) is according to tumor thrombus. Portal vein pylephlebitis: portal vein mural thickening and mural hyperenhancement with portal vein thrombus in the setting of sepsis. Teaching Points Portal vein tumor thrombus from hepatocellular carcinoma have to be considered whenever heterogeneous liver enhancement is seen in a cirrhotic liver or in a patient at risk for hepatocellular carcinoma. Obstruction of normal portal venous inflow ends in elevated arterial move in to the affected liver segments and incessantly leads to arterial part parenchymal hyperenhancement. Nonvisualization of a normal portal vein at imaging should prompt a search for a tumor that both obliterates the portal vein or that expands and distorts to the point that the portal vein is tough to acknowledge. Delayed imaging might present distinction material washout from the portal vein rather than enhancement similar to the blood pool. Discrete hepatocellular carcinomas must be sought, though the tumor may be obscured by the heterogeneous liver enhancement caused by portal vein obstruction. Management Portal vein tumor thrombus generally precludes healing liver transplantation for patients with hepatocellular carcinoma. Differential Diagnosis Tumor thrombus within the portal vein: may broaden the portal vein and enhance. Hepatoduodenal ligament lymph nodes or mass: usually less serpentine in shape and fewer enhancement. Teaching Points Cavernous transformation of the portal vein occurs as a consequence of extrahepatic portal vein thrombosis and occlusion. Numerous tortuous venous collaterals develop over a variable time course, starting from per week to a year. Collateral veins develop from biliary, gastric, pericholecystic veins, the partially recanalized portal vein, and portosystemic collateral channels that drain variably in to the left and right portal veins and the vasa vasorum. On ultrasound, circulate within collateral veins is generally hepatopetal, low velocity, and pretty monophasic, missing the slight pulsatility seen within the regular portal vein move. Portal venous thrombosis can be associated with hepatic parenchymal perfusion abnormalities from a compensatory increase in arterial influx or often bile duct obstruction due to mass impact by the collateral veins on the widespread duct. Atrophy of the left lateral phase and hypertrophy of the left medial phase and the caudate lobe can also happen in these instances. Causes of portal vein thrombosis embrace reduced portal circulate from underlying hepatic parenchymal illness, belly sepsis (infectious, stomach inflammation), and hypercoagulable states. Management Ninety percent of sufferers with cavernous transformation of the portal vein have portal hypertension. Differential Diagnosis Amebic Abscess: has very related imaging characteristics to a pyogenic abscess. Treated metastatic illness: affected person historical past of prior neoplasm and lack of fever, leukocytosis are clues to the right analysis. Biliary cystadenocarcinoma: encapsulated complicated cystic lesion occurring most commonly in middle-aged girls. Hepatic hydatid cyst: Cystic liver mass which will have varied appearances, including peripheral daughter cysts. Teaching Points Pyogenic liver abscess is a localized assortment of pus within the liver, typically from a polymicrobial bacterial infection. Pyogenic abscess accounts for 80 % of liver abscesses, with amebic abscess (from Entamoeba histolytica) being responsible for another 10 p.c, and fungal abscess (typically Candida) comprising the remaining 10 p.c. Biliary illness with ascending cholangitis and portal vein pylephlebitis from diverticulitis, appendicitis, or inflammatory bowel disease account for virtually all of circumstances within the Western world. Other causes included hepatic arterial septicemia, triggered perhaps by endocarditis or osteomyelitis, direct extension from perforated duodenal ulcer, or subphrenic abscess or from blunt or penetrating trauma. Patients current mostly with proper upper quadrant pain, malaise, and fever. If the infection spreads to the subphrenic region, right lower lobe atelectasis or a right pleural eff usion could additionally be present. Management Antibiotics and percutaneous abscess drainage with catheter placement is the process of choice for remedy of pyogenic liver abscess, with success charges of higher than ninety percent. For smaller abscesses, therapy with needle aspiration with antibiotics has also been proven to be efficient. History of major malignancy and correlation with prior studies is often diagnostic. Biliary cystadenocarcinoma: uncommon rim-enhancing cystic mass within the liver that may have thick mural septations or nodules, typically occurring in middle-aged girls. Pyogenic abscess: indistinguishable from amebic abscess by imaging characteristics. Subacute onset of symptoms and historical past of journey to an area the place the disease is endemic are helpful discriminators. Teaching Points Amebic liver abscess is essentially the most frequent extra-intestinal manifestation of Entamoeba histolytica an infection. Approximately 10 p.c of the world population is contaminated by contaminated consuming water, the vast majority in growing countries in Central America, India, and Southeast Asia. Patients typically current with acute to subacute signs of proper higher quadrant ache, tender hepatomegaly, and diarrhea with mucus. History of current travel to a region where the illness is endemic is critical in narrowing the differential diagnosis. Amebic abscesses are more common in the best hepatic lobe (72 percent), presumably due to the best lobe receiving the majority of its blood provide from the superior mesenteric vein. Potential problems include rupture via the diaphragm in to the chest with pulmonary abscess and hydropneumothorax, or intraperitoneal rupture with amebic peritonitis. Management Most uncomplicated amebic abscesses could be treated successfully with amebicidal drug remedy alone. An oral course of metronidazole for 10 days has been proven to be healing in ninety percent of uncomplicated circumstances, with resolution of signs inside three days in most sufferers. The cyst has a thick enhancing wall and contains a delaminated inside wall ("water lily" sign). Patients are sometimes acutely and severely unwell with fever and belly ache upon presentation. Minimal enhancement and central liquefaction is widespread, and these lesions usually mimic pyogenic infections. Hydatid cysts are composed of three histopathologic layers: the outer pericyst, the internal endocyst, and the interleaved ectocyst. On ultrasound, the imaging look is variable, ranging from cystic to strong appearing pseudotumors. Daughter cysts, peripheral calcification, and delaminated endocysts (water lily sign) may be current. Potential problems of hydatid disease embody cyst rupture, diaphragmatic and stomach wall involvement, peritoneal seeding, portal vein involvement, biliary communication, and hematogenous spread. Management Although beforehand not beneficial, following medical pretreatment with mebendazole, percutaneous drainage, and cyst sclerosis is now widely accepted. Complications, including superinfection of the treated cyst cavity and biliary communication, are attainable.
110 mg sinemet order with visa
Surgery is the therapy of selection for all malignant adrenal tumors; mitotane 6 tumor mattress radiation remedy is the really helpful adjuvant remedy for adrenocortical carcinomas treatment xanthoma 300 mg sinemet with mastercard. Incidentally found adrenal plenty ought to be evaluated for evidence of malignancy (size abro oil treatment sinemet 110 mg cheap mastercard. Allolio B, Fassnacht M: Clinical evaluation: Adrenocortical carcinoma: clinical replace, J Clin Endocrinol Metab ninety one:2027�2037, 2006. Assie G, Antoni G, Tissier F, et al: Prognostic parameters of metastatic adrenocortical carcinoma, J Clin Endocrinol Metab 92:148�154, 2007. Fassnacht M, Hahner S, Polat B, et al: Efficacy of adjuvant radiotherapy of the tumor bed on native recurrence of adrenocortical carcinoma, J Clin Endocrinol Metab 91:4501�4504, 2006. Groussin L, Bonardel G, Silvera S, et al: 18F-Fluorodeoxyglucose positron emission tomography for the prognosis of adrenocortical tumors: a potential research in 77 operated sufferers, J Clin Endocrinol Metab 94:1713�1722, 2009. Lacroix A: Approach to the affected person with adrenocortical carcinoma, J Clin Endocrinol Metab ninety five:4812�4822, 2010. Leboulleux S, Dromain G, Bonniaud G, et al: Diagnostic and prognostic worth of 18-fluorodeoxyglucose positron emission tomography in adrenocortical carcinoma: a prospective comparability with computed tomography, J Clin Endocrinol Metab 91:920�925, 2006. Pacak K, Eisenhofer G, Ahlman H, et al: Pheochromocytoma: recommendations for medical follow from the First International Symposium, Nat Clin Pract Endocrinol Metab 3:92�102, 2007. Terzolo M, Angeli A, Fassnacht M, et al: Adjuvant mitotane therapy for adrenocortical carcinoma, N Engl J Med 356:2372�2380, 2007. The most typical cause of central (secondary/tertiary) adrenal insufficiency is withdrawal of glucocorticoids after long-term use. Central adrenal insufficiency also can occur as a part of panhypopituitarism from massive pituitary tumors or their treatment with surgery and/or radiation remedy. Most patients report nonspecific signs similar to weak spot, fatigue, and anorexia. Many additionally complain of gastrointestinal signs corresponding to nausea, vomiting, vague abdominal pain, and constipation. Psychiatric signs and signs of orthostatic hypotension, arthralgias, myalgias, and salt craving are also reported. Hyperpigmentation, notably of the buccal mucosa and gums, is famous in most sufferers with primary adrenal insufficiency. The hyperkalemia is as a outcome of of mineralocorticoid deficiency, whereas the hyponatremia occurs mainly because of glucocorticoid deficiency. Hyponatremia is the end result of elevated vasopressin values with free water retention, shift of extracellular sodium in to cells, and decreased delivery of filtrate to the diluting segments of the nephron as a result of decreased glomerular filtration price. Patients usually show a normocytic normochromic anemia and may have eosinophilia and lymphocytosis. Fasting blood glucose is normally low-normal, however often sufferers can have fasting or postprandial hypoglycemia. Patients with coexisting kind 1 diabetes mellitus and adrenal insufficiency could experience greater frequency and severity of hypoglycemic episodes. In the outpatient setting, a low morning cortisol value (, three mg/dL) is adequate to diagnose adrenal insufficiency, and a high morning cortisol worth (. In most situations, a dynamic take a look at, the cosyntropin stimulation take a look at, is also carried out. If a person is receiving glucocorticoid therapy, the dose ought to be withheld (12 hours for hydrocortisone, 24 hours for prednisone) earlier than the test is carried out to avoid detection of synthetic glucocorticoids in the cortisol assay. Insulin-induced hypoglycemia (insulin tolerance testing) or metyrapone testing could additionally be utilized in these situations. After the biochemical prognosis of adrenal insufficiency, imaging may be performed in certain situations to help decide the trigger. Adrenal disaster must be suspected in patients with unexplained catecholamine-resistant hypotension or other extreme signs or signs in preserving with adrenal insufficiency. Symptoms of adrenal disaster are sometimes nonspecific-weakness, fatigue, nausea, vomiting, belly ache, fever, and altered mental status. If adrenal disaster is suspected, it must be treated aggressively as a outcome of, if left untreated, adrenal disaster is deadly. In addition, therapy should embody intravenous saline and glucose to right volume depletion, dehydration, and hypoglycemia. A seek for precipitating components and the underlying trigger needs to be carried out. In patients who (1) are hemodynamically unstable and unresponsive to vasopressors despite enough fluid resuscitation or (2) have signs or symptoms suggestive of adrenal insufficiency, random cortisol specimen ought to be collected, and a cosyntropin stimulation test performed immediately afterward. The cortisol level at which adrenal insufficiency must be recognized (a random stage of, 20 mg/dL, some other worth such as, 25 mg/dL, and/or an increment of 9 mg/dL after cosyntropin administration) is controversial. The reasons are concerns concerning the existence of a cortisol-resistant state in critically sick sufferers as a outcome of inflammatory cytokines, reduction in binding affinity to cortisol-binding globulin, and proinflammatory transcription elements. There is appreciable debate about the most acceptable use of glucocorticoids within the critical care setting. Although the outcomes of medical trials of glucocorticoid treatment for sepsis with out confirmed adrenal insufficiency have been mixed, a scientific review showed that 5 or more days of 300 mg/day or much less of hydrocortisone or its equal resulted in a significant reduction in 28-day all-cause mortality and hospital mortality. Some groups advocate using stress-dose steroids empirically in critically unwell sufferers with resistant hypotension, testing for adrenal insufficiency with a random cortisol measurement and cosyntropin stimulation testing, after which stopping stress-dose steroids if the tests for adrenal insufficiency are normal. All patients with persistent adrenal insufficiency require alternative with glucocorticoids, and occasionally with mineralocorticoids. Hydrocortisone is incessantly used in main adrenal insufficiency because it has some mineralocorticoid exercise. The usual dosage of hydrocortisone is 10 to 15 mg each morning and 5 to 10 mg within the afternoon. If further mineralocorticoid effect is important for persistent hyperkalemia and/or orthostatic hypotension, fludrocortisone zero. Many individuals with adrenal insufficiency experience considerably reduced subjective well being status and quality of life, increased fatigue, and depression. Work is being accomplished to develop sustainedrelease glucocorticoid formulations that higher approximate the natural diurnal cortisol sample. Adequate treatment for chronic adrenal insufficiency is monitored by taking a targeted historical past regarding general well-being and symptoms suggestive of orthostasis and obtaining blood pressure, weight, and electrolytes. It is necessary to keep away from the usage of extreme dosages of replacement glucocorticoids, which lead to iatrogenic Cushing syndrome, which in flip can outcome in unnecessary weight acquire, osteoporosis, hypertension, hyperglycemia, glaucoma, or avascular necrosis. The goal should be to use the smallest replacement dosage of glucocorticoids attainable that maintains regular electrolyte ranges and good high quality of life. Any medical stress, together with febrile illnesses, trauma, labor and supply, and diagnostic or surgical procedures, can precipitate an acute adrenal disaster in the patient with persistent adrenal insufficiency. Supplemental steroids ought to be used to stop adrenal crisis, however care should be taken to avoid unnecessary supplemental doses of glucocorticoids. Typically, the standard alternative dose is doubled or tripled for delicate to moderate infections and during labor and delivery. Doses also needs to be doubled or tripled for approximately 24 hours for dental surgical procedure, minor surgical procedure (cataract, laparoscopic), and invasive diagnostic procedures.
Discount sinemet 125 mg on line
Starting statins through the period of acute hospitalization could improve the continued use of those drugs after discharge medicine quetiapine 110 mg sinemet order with visa. In a really giant survey on more than 200 medications for ibs order sinemet 300 mg without a prescription,000 patients, late mortality fell by roughly 40%. For instance, b-blockade may have its greatest effects within the presence of coronary heart failure, with all-cause mortality lowered by 23%. The threat of hyperkalemia is substantial, and patients must be monitored carefully. It prevents reinfarction, stroke, and vascular mortality as shown in quite a few trials. Celecoxib in doses of 200 mg or more daily is associated with an increase in cardiovascular events. Two ex vivo studies have demonstrated a potential interaction of ibuprofen and probably naproxen, however not diclofenac or rofecoxib, when mixed with aspirin. Nonetheless, the hoped-for good factor about antiarrhythmic remedy on postinfarct mortality remains to be elusive, with b-blockers the only brokers showing clear-cut mortality discount. The use of Holter monitoring and invasive electrophysiologic testing has declined, and the most important inclusion criterion is the ejection fraction, albeit an imprecise measurement. Microvolt T-wave alternans seems essentially the most promising of the new approaches, but its ultimate position requires further clarification. Thus each time attainable, anticoagulation is required for both cardioversion or fee management. Spontaneous reversion is verapamil, or esmolol; generally digoxin or drug combinations). If not, think about pharmacologic cardioversion by intravenous ibutilide (risk of torsades) or high-dose amiodarone (125 mg/h, up to 3 g/24 h) or if no structural heart illness, flecainide or propafenone. Urgent Cardioversion � Required for speedy ventricular response not responding to pharmacologic brokers if myocardial ischemia, symptomatic hypotension, or heart failure (class1C). Elective Cardioversion,7 Days � Intravenous ibutilide or oral dofetilide (risk of torsades with both). Flecainide or propafenone only when no structural heart disease, with a b-blocker or verapamil to avoid a fast ventricular rate. Anticoagulation continued for no less than 3-6 mo, however normally indefinitely because many episodes are asymptomatic. Third policy: Cardiovert, observe on anticoagulation, begin antiarrhythmics for second episode. Under investigation: Dual-site atrial pacing; implantable atrial cardioverterdefibrillator. Classes of Recommendations (1-3) and levels of evidence (A-C) Other brokers that may also be given intravenously include flecainide, propafenone, sotalol, ibutilide, and high-dose amiodarone. In the presence of hypokalemia, digitalis toxicity or improper synchronizations, severe ventricular arrhythmias might occur. The danger of systemic thromboembolism is 1%-2%, and this may be decreased by anticoagulation. For urgent cardioversion, logic but no trial data would dictate intravenous heparin to cover the procedure. To cut back the chance of atrial stunning, oral verapamil could additionally be given earlier than and just after the cardioversion. This instantly visualizes thrombus within the left atrium or left atrial appendage, which, if discovered, contraindicates urgent cardioversion with out prior prolonged anticoagulation. Technical experience and expertise are essential for this method, as a outcome of the anatomy of the left atrial appendage is complicated and small thrombi can easily be overlooked. The logic for this line of remedy is that all the medicine that can be used to preserve sinus rhythm (flecainide, propafenone, sotalol, amiodarone, dofetilide, and dronedarone) have potentially 12 - Which Therapy for Which Condition The potential advantages of rhythm control are an enchancment within the high quality of life and exercise tolerance,276,277 with theoretical results on endothelial perform and platelet activation. In two different smaller European trials, fee control was again similar in consequence to rhythm control. Other medicine which might be useful for pharmacologic rate management include dronedarone and amiodarone. Strict price management is a resting coronary heart fee lower than eighty beats per minute (bpm) and a heart rate lower than one hundred ten bpm with minor train. In regard to cardiovascular occasions, the technique of lenient rate control was noninferior, suggesting that we should favor a policy of treating the patient and not the rate. When fee management is unsatisfactory, tachycardia-induced ventricular dysfunction is a priority. Working down the alternatives, the final drug is normally amiodarone, failing which catheter ablation follows. Renin-angiotensin blockade helps to reduce recurrences with good theoretical explanations,294 and benefits comorbidities similar to heart failure and hypertension. It is unlikely, nonetheless, that these agents will play more than an adjunctive position. Moreover, there are numerous drug interactions which will prohibit using dofetilide. A driving pressure underlying the suggestions for antiplatelet and anticoagulant remedy is the stratification of patients according to their risk of bleeding and stroke. The conclusion is that there was substantial differences among the many numerous schemes and none have been optimal. The key to remedy is to individualize and balance the chance of stroke versus the risk of bleeding. The limitations of vitamin K antagonists are well known, together with a narrow therapeutic range, gradual "onset" and "offset" of action, quite a few meals and drug interactions, the inference of genetic variability and clearance, and the effect of concurrent diseases in pharmacokinetics and pharmcodynamics. This requires constant and frequent monitoring for anticoagulant effect and frequent dose changes. The direct thrombin inhibitor dabigatran etexilate (Pradaxa) is launched in the United States at doses of a hundred and fifty mg twice a day and 75 mg twice a day in patients with an estimated glomerular filtration price of lower than 30 mL/min, however in Europe and Canada the 110-mg twice-daily dose is also available. Superiority was demonstrated solely in evaluation that in contrast "as handled" patients however not in the intention-2-3 evaluation. Surgical procedures and radiofrequency ablation are invasive approaches to rhythm management which are important advances. The major indication for the surgical maze process is in patients undergoing cardiac surgical procedure for different indications. Increasing experience, new imaging methods, and advances in electromechanical mapping will likely result in further improvements to the general success of the process. Complication rates are declining, but the potential for severe complications corresponding to thromboembolism together with stroke, tamponade, pulmonary vein stenosis, phrenic nerve harm, and ateroesophageal fistula occur in approximately 2%-3% of patients. Operator experience might be an essential component of general success and security. Satisfactory control of the ventricular price could additionally be extraordinarily troublesome to obtain, however flutter is definitely converted by a lowenergy countershock. Patients with "typical atrial flutter" take pleasure in a very excessive success price with radiofrequency ablation of the flutter circuit.
125 mg sinemet generic free shipping
The mixture of focal consolidation or mass with satellite nodules has been termed the "galaxy signal treatment uterine cancer sinemet 125 mg buy on-line. Lung home windows (A) present nonspecific consolidation in a patient with focal symptoms 0f diabetes sinemet 300 mg discount with visa, chronic consolidation. Soft tissue home windows (B) show areas of fat attenuation (arrows) in consolidation suitable with lipoid pneumonia. Lipoid Pneumonia with Low-Attenuation Consolidation Lipoid pneumonia is a rare reason for consolidation. The two malignancies that may present with chronic consolidation embody invasive mucinous adenocarcinoma and lymphoma. High decision lung computed tomography: regular anatomic and pathologic findings. These include lung destruction as a result of emphysema, decreased lung perfusion, cyst formation, and airway dilatation. Airway dilatation, or bronchiectasis, is normally identifiable as such and shall be discussed in the subsequent chapter. In general, the severity of emphysema correlates with the length of time and amount a patient has smoked. Smoke induces lung destruction by inflicting continual irritation in and around small airways (respiratory bronchiolitis). Because these small airways are centrilobular in location, emphysema associated with smoking is predominantly centrilobular in distribution. As lung destruction becomes more intensive, emphysema might contain the entire pulmonary lobules. These lucencies are most likely to predominate in the upper lobes and are most extreme in the central lung regions. It is seen in the peripheral lung, adjacent to the mediastinum, and adjacent to fissures. A bulla is outlined as a sharply defined space of emphysema measuring greater than 1 cm in diameter. In another affected person with a left lung transplant for panlobular emphysema, the abnormal, markedly hyperinflated and lucent native right lung can be contrasted with a normal appearing transplanted left lung. In cases of vascular illness, similar to persistent pulmonary embolism, decreased perfusion is as a outcome of of stenosis or occlusion of pulmonary arterial branches. In circumstances of airways disease, stenosis or obstruction of the abnormal airways leads to decreased air flow and hypoxia in the downstream lung. This finding is vital in making the prognosis of mosaic perfusion as a explanation for patchy lung attenuation. Geographic Areas of Decreased Lung Attenuation With mosaic perfusion, areas of heterogeneous attenuation tend to be geographic and sharply demarcated. Heterogeneous lung density with geographic areas of decreased lung attenuation (arrows) is present in a patient with constrictive bronchiolitis due to neuroendocrine hyperplasia. This sharp demarcation between opaque and lucent lung means that the lucent lung is irregular. Vessels in lucent areas seem small in comparability to vessels in the denser areas. On event, however, floor glass opacity presents with geographic abnormalities. For instance, viral infections or alveolar proteinosis might current with geographic areas of ground glass opacity. Air Trapping on Expiratory Imaging When mosaic perfusion is due to airways disease, lucent lung regions usually show air trapping on expiratory imaging. When airways disease is current, air trapping causes affected regions to present little or no improve in attenuation on expiratory images. Patchy perihilar areas of elevated lung attenuation are current in a affected person with pneumocystis pneumonia. The edges of the areas of ground glass opacity are ill-defined, quite than sharply demarcated. There may be different findings current such as nodules, tree-in-bud, bronchiectasis, airway wall thickening, air trapping, or pulmonary hypertension that suggest a specific diagnosis. While geographic areas of heterogeneous lung attenuation are normally as a outcome of mosaic perfusion, sometimes, floor glass opacity may have sharply demarcated borders. The marked distinction in attenuation between affected and unaffected lung on this case can be uncommon for mosaic perfusion, and frank consolidation can also be seen. Differentiating Airways versus Vascular Causes of Mosaic Perfusion In most instances, a distinction could be made between mosaic perfusion resulting from airways illness and vascular illness. Stability of Mosaic Attenuation Over Time Ground glass opacity usually changes in distribution or severity over time, except it is because of fibrosis. The vessels are significantly smaller in the abnormally lucent lung (yellow arrow) as compared with the normal opaque lung (red arrow). Geographic areas of decreased lung attenuation are present on the inspiratory images. Expiratory images verify air trapping within the lucent lung and a normal increase in density (yellow arrow) of the opaque lung (B) on this affected person with constrictive bronchiolitis because of pulmonary graft versus host illness. Vascular illness, in contradistinction, sometimes demonstrates bigger, usually peripheral areas of decreased attenuation and not utilizing a lobular look. Headcheese is a sausage made from the chopped and boiled elements of the pinnacle of an animal, usually a hog. It seems as a mosaic of different-appearing meats, of various colours and textures. The mixture of ground glass opacity and mosaic perfusion in the same patient, each in significant quantities, constitutes the headcheese signal. Three attenuations (or more) can also be present, representing a combination of regular lung, opaque lung (ground glass opacity), and lucent lung (mosaic perfusion). The attenuation variations are accentuated on expiratory scans by which both the traditional and opaque lung will turn out to be denser, but the areas of mosaic perfusion will keep lucent. The headcheese signal is seen in patients with mixed obstructive and infiltrative problems. The obstructive abnormality is manifested by mosaic perfusion associated with small airways illness. There are a restricted number of issues which have both a major obstructive and infiltrative component (Table 5. In this case, mosaic perfusion must be ignored in phrases of differential prognosis and the emphasis should be positioned on the large airway abnormalities. Air trapping in a patient with mosaic perfusion indicates the presence of airways disease. There is a rise in attenuation of the more lucent lung when evaluating inspiratory (A, arrow) and expiratory (B, arrow) pictures. The morphology of the lucent lung in mosaic perfusion may differ between airways and vascular illness. In airways disease (A), the lucent lung usually seems lobular (arrow) compared with the larger, peripheral, non-lobular appearance (arrows) in vascular disease (B).
Sinemet 125 mg generic with mastercard
Inflammation medicine runny nose 125 mg sinemet cheap with visa, aspirin and the risk of heart problems in apparently healthy men treatment leukemia sinemet 300 mg best. Aspirin-resistant thromboxane biosynthesis and the danger of myocardial infarction, stroke, or cardiovascular death in sufferers at high risk for cardiovascular events. Aspirin and clopidogrel drug response in sufferers undergoing percutaneous coronary intervention: the function of dual drug resistance. Doubleblind trial of aspirin in main prevention of myocardial infarction in patients with secure chronic angina pectoris. Association of aspirin use with major bleeding in sufferers with and without diabetes. Guidelines for the primary prevention of stroke: a suggestion for healthcare professionals from the American Heart Association/American Stroke Association. Short-term results of daily aspirin on most cancers incidence, mortality, and non-vascular demise: analysis of the time course of risks and advantages in 51 randomised managed trials. Effect of daily aspirin on risk of cancer metastasis: a study of incident cancers throughout randomised managed trials. A comparison of two doses of aspirin (30 mg vs 283 mg a day) in sufferers after a transient ischemic assault or minor ischemic stroke. Low-dose and high-dose acetylsalicylic acid for sufferers present process carotid endarterectomy: a randomised controlled trial. Effects of long-term treatment with angiotensin-converting-enzyme inhibitors in the presence or absence of aspirin: a systematic evaluate. Clinical effects of early angiotensin-converting enzyme inhibitor treatment for acute myocardial infarction are related within the presence and absence of aspirin: systematic overview of individual knowledge from 96,712 randomized sufferers. Effects of acetylsalicylic acid on peripheral hemodynamics in sufferers with persistent coronary heart failure handled with angiotensin-converting enzyme inhibitors. Meta-analysis of randomized and registry comparisons of ticlopidine with clopidogrel after stenting. Impact of the diploma of peri-interventional platelet inhibition after loading with clopidogrel on early medical outcome of elective coronary stent placement. Impact of platelet reactivity on medical outcomes after percutaneous coronary intervention a collaborative meta-analysis of particular person participant data. Prevention of premature discontinuation of twin antiplatelet therapy in sufferers with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with illustration from the American College of Physicians. Addition of clopidogrel to aspirin in forty five,852 sufferers with acute myocardial infarction: randomised placebo-controlled trial. Bridging antiplatelet therapy with cangrelor in patients present process cardiac surgical procedure. Oral antiplatelet remedy for atherothrombotic disease: present evidence and new directions. Readministration of abciximab is as efficient as first time administration with similar risks: outcomes from the ReoPro Readministration Registry (R3) [abstract]. Mortality at 1 year for the direct comparability of tirofiban and abciximab during percutaneous coronary revascularization: do tirofiban and ReoPro give comparable efficacy outcomes at trial 1-year follow-up. Tirofiban as adjunctive remedy for acute coronary syndromes and percutaneous coronary intervention: a meta-analysis of randomized trials. American Heart Association/American College of Cardiology Foundation guide to warfarin therapy. Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in patients with atrial fibrillation and prior stroke or transient ischemic attack. Racial/ethnic variations within the threat of intracranial hemorrhage amongst sufferers with atrial fibrillation. Randomized trial of genotype-guided versus commonplace warfarin dosing in sufferers initiating oral anticoagulation. The optimal intensity of vitamin K antagonists in patients with mechanical heart valves: a meta-analysis. Effect of elevated warfarin use on warfarin-related cerebral hemorrhage: a longitudinal population-based examine. Risk of osteoporotic fracture in aged patients taking warfarin:, results from the National Registry of Atrial Fibrillation 2. Comparison of the efficacy and safety profiles of intravenous vitamin K and contemporary frozen plasma as treatment of warfarin-related over-anticoagulation in sufferers with mechanical heart valves. Atherothrombosis-wave goodbye to mixed anticoagulation and antiplatelet remedy Long-term, low-intensity warfarin therapy for the prevention of recurrent venous thromboembolism. Validation of scientific classification schemes for predicting stroke: results, from the National Registry of Atrial Fibrillation. Refining medical risk stratification for predicting stroke and thromboembolism in atrial fibrillation utilizing a novel threat factor-based approach: the Euro coronary heart survey on atrial fibrillation. Stroke with intermittent atrial fibrillation: incidence and predictors throughout aspirin remedy. Effect of persistent kidney disease on warfarin management in a pharmacist-managed anticoagulation clinic. Warfarin-related nephropathy happens in sufferers with and with out persistent kidney illness and is associated with an elevated mortality rate. Comparison of low-intensity warfarin remedy with conventional-intensity warfarin therapy for long-term prevention of recurrent venous thromboembolism. Prevention of stroke and systemic embolism with rivaroxaban compared with warfarin in sufferers with non-valvular atrial fibrillation and average renal impairment. Low-dose fondaparinux in suspected heparin-induced thrombocytopenia, in the critically sick. Efficacy and safety of the low-molecular weight heparin enoxaparin in contrast with unfractionated heparin throughout the acute coronary syndrome spectrum: a meta-analysis. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty. Efficacy and security of Fondaparinux versus Enoxaparin in patients with acute coronary syndromes present process percutaneous coronary intervention. Thrombolysis and myocardial salvage: outcomes of scientific trials and the animal paradigm-paradoxic or predictable Indications for fibrinolytic therapy in suspected acute myocardial infarction; collaborative overview of early mortality and major morbidity results from all randomised trials of greater than a thousand sufferers. Pharmacological facilitation of main percutaneous coronary intervention for acute myocardial infarction: is the slope of the curve the form of the longer term An international randomized trial comparing 4 thrombolytic methods for acute myocardial infarction. Comparative evaluation of the exercise and content material of various strep to , kinase preparations. Clinical results of anticoagulant remedy in suspected acute myocardial infarction: systematic overview of randomised trials. A comparison of pharmacologic therapy with/without timely coronary intervention vs.
Purchase sinemet 125 mg mastercard
Fluid and fats stranding may be current in the anterior perirenal house of the retroperitoneum symptoms pulmonary embolism 300 mg sinemet generic mastercard. It is necessary to intently examine the adjoining organs such because the pancreas symptoms hyperthyroidism sinemet 110 mg low cost, gallbladder, liver, and spleen in addition to the vasculature for extra websites of damage. Management Duodenal hematomas with out perforation are usually managed conservatively. A extra inferior image (right) exhibits trace fluid in Morison pouch and along the liver tip (arrow) with wall thickening and fat stranding of the gastric antrum and duodenal bulb (arrowheads). Differential Diagnosis Perforated appendicitis or diverticulitis: unusual to see free air in the left anterior subphrenic house. Bowel wall thickening, fat stranding, and fluid with pockets of extraluminal air are typically concentrated within the lower stomach or pelvis. Perforated small bowel diverticulum: could show findings just like perforated peptic ulcer disease. Teaching Points Despite the decreased incidence of peptic ulcer illness because of improved prevention and treatment, perforated ulcers stay a serious life-threatening complication. The website of perforation can be advised primarily based on several observations: the distribution of intraperitoneal air, the presence of fluid and fat stranding, and the placement of fats stranding and thickening of the affected bowel. When this sign is present, perforations are normally in the stomach or small bowel. In general, when large quantities of free intraperitoneal air are current in the absence of instrumentation, the most typical source of the free air is a gastric or duodenal ulcer perforation. Management Most patients with perforated peptic ulcer will need emergency surgery such as a patch repair or resection. The mesenteric fats is asymmetrically expanded, displaces bowel loops, and encases engorged peri-enteric vessels, that are also called the vasa recti (long arrow). Differential Diagnosis Infectious enteritis: imaging findings usually replicate acute irritation corresponding to mucosal hyperenhancement. Graft versus host illness: look and distribution of the abnormalities could also be similar, however the affected person should have a historical past of allogenic stem cell transplantation. Radiation enteritis: early stages may show inflamed bowel within the distribution of the irradiated field that may produce strictures. Teaching Points Crohn illness is a chronic inflammatory dysfunction typified by transmural inflammation and multifocality that will involve the alimentary tract at any stage, but has a predilection for the terminal ileum and colon. Imaging helps set up the analysis and characterize illness extent, severity, and problems. Active irritation is characterised by mucosal and muscular hyperenhancement, a thickened, edematous bowel wall, and engorged vasa recta. It is essential to acknowledge complications such as sinus tracts, fistulas, and abscesses, in addition to any luminal narrowing with pre-stenotic dilatation that signifies small bowel strictures. The latter may develop from mural fibrosis or mural edema within the setting of active disease. Submucosal fat deposition and proliferation of mesenteric fat, so referred to as "creeping fats" or "fibrofatty proliferation," could also be related to chronically concerned segments of small bowel. Management Disease distribution and the presence or absence of mesenteric problems must be reported to have the ability to guide medical (antibiotic and immunosuppressive) and surgical remedy. It is useful to observe the placement and length of every strictured section as properly as the presence of sinus tracts and abscesses for the purpose of interventional and surgical planning. Differential Diagnosis Small bowel lymphoma: normally extra nodular or concentric bowel mass with associated lymphadenopathy. Small bowel adenocarcinoma: uncommon and should present as polypoid mass or irregular "apple-core" lesion, usually in the duodenum or jejunum, and may be associated with inflammatory enteritis. Ischemic enteritis: presents acutely with segmental bowel wall thickening and attainable pneumatosis or mural nonenhancement, sometimes with superior mesenteric artery or vein thrombus. Infectious enteritis: other pathogens that characteristically contain the distal ileum and trigger stricturing corresponding to Tuberculosis may have a similar look. Graft-versus-host disease: history of bone marrow transplant is critical for the prognosis. Teaching Points Crohn disease is a continual, transmural inflammatory course of that may happen in any segment of bowel, however most commonly impacts the terminal ileum. The age of onset is bimodal, with the primary peak occurring at ages 15 to 30 and a smaller second peak at ages 60 to eighty. Characteristic imaging findings embody discontinuous segments of bowel wall thickening, mucosal or mural hyperenhancement resulting in a "stratified" appearance that shows inner mucosal hyperenhancement and hypoattenuation of the adjoining, edematous submucosa. Adjacent mesenteric modifications such as fibrofatty proliferation, lymphadenopathy and mesenteric hypervascularity (known as the comb signal due to its look in imaging) are often current. Stricturing of involved segments may occur, even after profitable therapy of acute flares. Resection of diseased segments of bowel and fistulae could additionally be undertaken, but recurrent illness is frequent. Delayed small bowel follow-through radiograph from another patient shows skinny, linear collections of barium (arrow) in the intestinal tract of the worm. Trichuris trichiura: roundworm that inhabits the colon, attaching to and superficially invading the mucosa. Most persons are asymptomatic but can current with obscure abdominal pain, nausea, vomiting, dietary deficiency, or a history of passing worms orally or rectally. Complications of ascariasis embrace mechanical small bowel obstruction, volvulus, or intussusception. They can even lodge within the pancreaticobiliary ductal system, inflicting pancreatitis, cholecystitis, or liver abscess. On barium research, an Ascaris is an elongated, worm-like filling defect in the small bowel. On ultrasound, worms are hypoechoic, sometimes writhing tubular buildings with echogenic walls, with the digestive tract of the worm forming two comparable echogenic traces. Management Stool samples are diagnostic for ascariasis, which is treated with albendazole. Dilated small bowel proximal to the ileum suggests partial small bowel obstruction. Differential Diagnosis Crohn illness: could also be indistinguishable from tuberculosis on barium studies. Cecal contraction and narrowing is often extra extensive in tuberculosis than in Crohn illness. Lymphoma: has more easy mass impact and fewer associated mucosal modifications corresponding to ulceration, nodularity. Adenocarcinoma: may type fistula to adjacent segments of bowel if perforation occurs.
Diseases
- Muscle-eye-brain syndrome
- Deafness nephritis ano rectal malformation
- Trichothiodystrophy sun sensitivity
- X-linked mental retardation and macroorchidism
- Sacral defect anterior sacral meningocele
- Phosphomannoisomerase deficiency
Generic sinemet 125 mg with mastercard
When these deposit within the walls of pulmonary vessels medicine wheel native american 300 mg sinemet order visa, capillaritis outcomes that will result in treatment diabetic neuropathy sinemet 125 mg effective diffuse pulmonary hemorrhage. A combination of ground glass opacity and clean interlobular septal thickening is seen in a affected person with pulmonary hemorrhage from vasculitis. Other causes of the crazy paving pattern in the acute setting include edema, atypical an infection, and diffuse alveolar harm. Computed tomography of diffuse pulmonary haemorrhage with pathological correlation. They are finest thought of as reactions to lung harm, presenting with particular histologic patterns. They are loosely unified by several characteristics including medical presentation, radiographic manifestations, and pathologic look and could also be idiopathic or related to particular ailments. They have been redefined and reclassified a number of occasions as an understanding of their patterns has been refined. While some of the phrases in the authentic classification have remained the same, others have been modified or deleted. Cases that are predominantly inflammatory end in floor glass opacity and consolidation. The interstitial pneumonias present with varying levels of inflammation and fibrosis. Two patients with nonspecific interstitial pneumonia from connective tissue disease are depicted. These findings mirror irreversible lung scarring that may be unresponsive to remedy. C ha pter 9 l the Interstitial Pneumonias 131 9 central in axial distribution and present sparing of the inferior costophrenic angles. A diffuse or central axial distribution is atypical for an interstitial pneumonia and suggests alternative ailments similar to hypersensitivity pneumonitis or sarcoidosis. Honeycombing results in the presence of clustered, cystic airspaces, with well-defined partitions, usually 3 to 10 mm in diameter, and predominating in the subpleural lung. As with the general extent of abnormalities, honeycombing, when present, is most extreme and extensive at the lung bases. A assured analysis of honeycombing (arrows) may be made in this case despite the mild abnormalities. Ground glass opacity is often seen in lung areas that additionally show findings of fibrosis. The findings of fibrosis are often patchy in distribution, however involve the posterior and subpleural lung to the best degree. According to criteria just lately agreed upon by American, European, Japanese, and Latin American societies (Table 9. Coronal reformat (D) and coronal minimum intensity projection (E) photographs affirm the basilar distribution of illness. A typical usual interstitial pneumonia sample is current, manifested by patchy subpleural honeycombing. It has been recommended that in such a case, a careful consideration of all knowledge by a multidisciplinary group of lung disease experts is critical. Patients with connective tissue disease usually have additional medical manifestations of a systemic dysfunction. Small centrilobular nodules in the peripheral lung, reflecting peribronchiolar fibrosis, have been described with asbestosis, but that is an uncommon finding and is usually seen in early illness. In this affected person with hypersensitivity pneumonitis, inclined scans show a central and mid-lung predominance of abnormalities. Expiratory image by way of the lung base exhibits patchy bilateral air trapping (arrows). Sarcoidosis is often higher lobe predominant and central or peribronchovascular in distribution. An upper lung and peribronchovascular distribution of fibrosis is typical of persistent sarcoidosis. This is in distinction to most of the interstitial pneumonias which might be usually peripheral and basilar predominant. Because of the central and higher lobe distribution on this case, it might be learn as inconsistent with traditional interstitial pneumonia. This is in distinction to ordinary interstitial pneumonia in which honeycombing is usually a major factor of the abnormality present. In every of these cases, floor glass opacity (arrows) is essentially the most significant abnormality. Findings of fibrosis, corresponding to traction bronchiectasis, are absent or mild in severity. Ground glass opacity may also be current, however this will likely mirror superimposed cellular disease. In each of those instances, irregular reticulation (blue arrows) and traction bronchiectasis (red arrows) are the predominant findings. Findings of fibrosis (reticulation, traction bronchiectasis, (c) 2015 Wolters Kluwer. Coronal reformatted picture (D) and coronal minimal intensity projection (E) confirm the basilar distribution of findings. More extreme traction bronchiectasis and irregular reticulation is current in a patient with scleroderma. The quick subpleural lung is much less abnormal than lung 1 cm away from the pleura. It was previously often known as bronchiolitis obliterans with organizing pneumonia, however this time period has been dropped for a number of reasons. Second, this time period avoids confusion with airways diseases, specifically bronchiolitis obliterans. This is a nonspecific finding, however in a smoker with persistent signs, desquamative interstitial pneumonia is the favored prognosis. Peripheral and peribronchovascular consolidation, usually with a nodular or mass-like look, and irregular margins, is seen bilaterally. This manifests as a ring or partial ring of consolidation surrounding a central region of clearing or floor glass opacity. Organizing pneumonia typically presents with consolidation as the predominant abnormality. A peripheral rim of consolidation (yellow arrows) surrounding a central space of clearing or floor glass opacity (red arrows) known as the atoll or reversed halo signal. Patchy subpleural and peribronchovascular mass-like areas of irregular consolidation are present. There are multiple possible causes of organizing pneumonia, certainly one of which is drug toxicity. If imaged early in its course, the abnormalities could have a peripheral distribution, however then quickly turn out to be diffuse in nature.
Discount sinemet 300 mg online
Infectious colitis: could additionally be radiographically indistinguishable from different colitides and requires stool sampling for diagnosis medicine remix 300 mg sinemet discount overnight delivery. Inflammatory bowel disease: Crohn illness and ulcerative colitis are most likely to treatment 2 lung cancer best sinemet 300 mg have much less wall thickening, pericolonic irritation, and ascites. Teaching Points Pseudomembranous colitis must be suspected in any patient with diarrhea or other abdominal symptoms who has been present process antibiotic remedy within latest months. Broad-spectrum antibiotics allow Clostricum difficile to proliferate and elaborate a toxin that causes the colitis. Low attenuation mural thickening similar to mucosal and submucosal edema can seem as a "target" when the bowel is seen in cross-section on intravenous contrasenhanced images, and will give the looks of an "accordion" when seen longitudinal to the bowel. Management Surgical intervention with colectomy could also be required for refractory cases or when toxic megacolon or pneumatosis complicate the illness. Pseudomembranous colitis: spectrum of imaging findings with clinical and pathologic correlation. Differential Diagnosis Neutropenic colitis (typhlitis): colonic wall thickening and pericolonic irritation involving the cecum and ascending colon. Tuberculosis: could have indolent presentation and low-density mesenteric lymph nodes. Inflammatory bowel illness: often reveals rectal involvement with out skip lesions. Initial an infection in an immunocompetent host is often gentle and may be subclinical. Mucosal ulcerations are frequent and will erode in to adjacent blood vessels with resultant hemorrhage in to the bowel wall or lumen. Management Treatment with the antiviral treatment gancyclovir is first-line remedy for immunocompetent and immunocompromised sufferers. Cytomegalovirus Colitis in Acquired Immune Deficiency Syndrome: Radiologic Spectrum. Prevalence, Detection Rate and Outcome of Cytomegalovirus Infection in Ulcerative Colitis Patients Requiring Colonic Resection. Crohn disease: Features include discontinuity of disease, terminal ileal involvement, strictures, fistulas, and lymph node enlargement. Teaching Points Causes of neutropenia include drug reactions, autoimmune diseases, infections, and hematologic malignancies. Neutropenic colitis stays poorly understood and pathologically is represented by compromised wall integrity with subsequent bacterial or fungal invasion. Severe instances may end in any combination of abscess formation, sepsis, intestinal necrosis, hemorrhage, and perforation. Management In the setting of a history of neutropenia, a immediate prognosis is crucial. Treatment with supportive therapy including broad-spectrum antibiotics and supplemental diet is necessary. Gastrointestinal Complications within the Neutropenic Patient: Characterization and Differentiation. Differential Diagnosis Infectious colitis or inflammatory bowel illness: usually cause vital bowel wall thickening and a goal or double halo sign from submucosal edema and mucosal hyperenhancement. Other causes of pneumatosis embody: publish invasive procedure such as colonoscopy, idiopathic, cystic fibrosis, scleroderma, chemotherapeutic agents, and steroid remedy. Serum lactate could additionally be elevated, and the patient may have an elevated white cell count and a metabolic acidosis. Possible causes embrace systemic hypoperfusion, venous thrombosis, arterial occlusion, embolism, and vasculitis. Ischemic colitis tends to happen in the watershed space of the colon: splenic flexure or rectosigmoid junction. Differential Diagnosis Diverticulitis: may present focal colonic wall thickening, however usually associated with diverticulosis and signs of sepsis with acute signs. Teaching Points Left-sided and sigmoid colon adenocarcinomas are far more widespread than right-sided colon cancers. Typical scientific signs of left-sided cancers embrace reduction in stool caliber, bright purple blood per rectum, and colonic obstruction. Due to the bigger caliber of and the more liquid consistency of stool in the proper colon, findings of anemia and weight reduction are more frequent with proper than with left colon cancers. Of note, colon cancer may be related to upstream or downstream colonic wall thickening, which may mimic a primary inflammatory quite than malignant process. For definitive diagnosis, colonoscopy could additionally be required after acute signs resolve. However, if colonic obstruction is current, surgical procedure could additionally be required previous to other remedy. There is a polypoid mass alongside the posterior facet of the cecal wall that extends in to the cecal lumen (arrow in proper image). For example, related diverticula, an inflamed appendix, or findings that would suggest Crohn disease. Teaching Points Perforation is likely one of the major complications of colorectal adenocarcinoma. Perforations could result in abscesses, fistulas to adjacent organs such because the bladder, abdomen, and adjacent segments of bowel, pneumoperitoneum, or pneumoretroperitoneum. Perforated carcinomas could also be tough to distinguish from diverticulitis with perforation. Observation of the next options could additionally be helpful to favor carcinoma over diverticulitis: asymmetric wall thickening of the colon, delicate tissue mass-like thickening of the colon wall, or the presence of an intraluminal polypoid mass. Inflammatory stranding, lymphadenopathy, and pericolonic fluid could additionally be current in both conditions. Management the management of perforated colon most cancers may embrace diverting colostomy with partial or complete colectomy carried out at a single operation or over multiple operations. Percutaneous drainage of the abscess and endoscopic stenting of the colon are adjunctive or various choices relying upon scientific condition of the patient. Psoas abscess and cellulitis of the proper gluteal region ensuing from carcinoma of the cecum. Differential Diagnosis Cecal volvulus: the dilated loop of colon directed towards left higher stomach, often with only one air-fluid degree. Rectal gasoline is often seen, particularly on a proper lateral decubitus or prone lateral view. Large bowel obstruction as a outcome of different trigger: dilated small bowel and colon proximal to the obstructing lesion. Teaching Points Sigmoid volvulus is the third main trigger of huge bowel obstruction after diverticulitis and carcinoma in Western countries. In Western international locations sigmoid volvulus is usually acquired from long-standing constipation, Parkinson illness, Alzheimer disease, or persistent debilitation. Radiographic findings include a "espresso bean" or "kidney bean" sign referring to a closed loop of sigmoid distended with fuel, with apposed medial partitions of dilated bowel forming an oblique line that resembles the cleft of a espresso bean. The dilated sigmoid classically points to proper higher quadrant, but could also be midline or left ward. Moderate or severe dilatation of the sigmoid with a sigmoid transition level is a extra specific discovering.
Purchase sinemet 300 mg without prescription
Because the entire following may be associated with stones medications used for fibromyalgia sinemet 300 mg effective, ask about use of guaifenesin medicine the 1975 sinemet 300 mg order on-line, ephedrine, indinavir, triamterene, sulfonamides, acyclovir, and nutritional vitamins A, C, and D. Determine fluid consumption and sources of extra calcium, salt, oxalate, uric acid, and protein. Physical examination is mostly not useful besides during acute disease (see query 28). Have the patient strain all urine and save the stone, if handed, for stone evaluation. More than 50% of stones in the proximal ureter and 75% of stones within the distal ureter lower than 5 mm move spontaneously. Order a blood chemistry panel that includes serum sodium, potassium, chloride, carbon dioxide, creatinine, calcium, albumin, phosphorus, magnesium, and uric acid. If the affected person has continued signs, if the stone is bigger than 5 mm, or if obvious obstruction is present, seek the advice of a urologist and plan for a more in depth analysis. Include a 24-hour urine take a look at for creatinine, sodium, calcium, phosphorus, magnesium, oxalate, citrate, and uric acid. Consider repeating the 24-hour urine test to give attention to abnormalities 6 weeks after medical intervention. Pain can be managed with nonsteroidal antiinflammatory medication, however opioid analgesics may be essential to deal with acute pain exacerbations. Calcium channel blockers corresponding to extended-release nifedipine and alpha-blockers similar to tamsulosin, doxazosin, and terazosin may facilitate stone passage by decreasing ureteral spasm and enhancing peristalsis throughout acute colic episodes. Patients with symptomatic stones, stones bigger than 5 mm, or a quantity of stones should be referred for nephrologic or urologic analysis. Unless contraindicated, stopping stone recurrence requires 2 to 3 L/day of fluid to improve urine output to greater than 2 L/day; no more than 2 g/day of sodium; zero. If a ureteral stone is smaller than 10 mm, alpha1-blockers or calcium channel blockers might help its passage. Prevention of stone recurrence contains day by day consumption of 10 to 12 8-ounce glasses of fluid, increased ingestion of citrate-containing drinks, a thousand mg/day of dietary calcium, zero. Avoid grapefruit juice, scale back oxalate and ascorbic acid to lower than one hundred mg/day for calcium oxalate stones, and use calcium supplements provided that dietary calcium is insufficient to enable intake of 800-1000 mg of calcium per day-calcium citrate most popular. Although potassium citrate is preferred for urinary alkalization and citrate replacement, citrus drinks such as lemon, lime, and orange juice may be substituted. Refer patients to a urologist for continued pain, obstruction, an infection, severe bleeding, fever, or renal dysfunction. Crystals are normally absent in warm, freshly voided urine but, if current, suggest a prognosis. However, most urine specimens cool earlier than examination, and crystals may kind in normal urine with time and cooling. Thus, by the point urine is usually examined, the discovering of crystalluria could have little medical significance. An exception is the presence of cystine crystals, which are diagnostic of cystinuria. Calcium oxalate monohydrate crystals may be dumbbell-shaped, needle-shaped, or oval, with the final resembling pink blood cells. Calcium oxalate dihydrate crystals are pyramid-shaped and have an envelope appearance. Calcium phosphate and uric acid crystals are too small for traditional mild microscopic decision and seem like amorphous particles. Less generally, uric acid dihydrate crystals may be rhomboid-shaped or resemble the four-sided diamonds on a deck of playing cards. However, the presence of cystine crystals, which are flat, hexagonal plates resembling benzene rings, at all times means cystinuria. Struvite (magnesium ammonium phosphate) crystals are rectangular prisms that resemble coffin lids. Ultrasonography reveals the size and location of bigger stones, is sensitive for diagnosing obstruction, and may be greatest when radiation must be averted, as in pregnancy. However, the preliminary radiographic process of choice for stone evaluation requires no patient preparation and is simple, sensitive, particular, and correct. Sodium citrate will increase urinary sodium and calcium, and in alkaline urine, sodium urate could improve calcium stone formation. Cystine stone formers require higher fluid intake to scale back urinary cystine beneath its solubility limit of 200 to 250 mg/L. Fluid and potassium citrate typically are the only therapy necessary for uric acid stones if uricosuria is lower than 800 mg/day. Use allopurinol with potassium citrate if uric acid stones continue or hyperuricemia is more extreme. Use the bottom dosage essential to attain the desired impact and keep away from side effects. Always use drug remedy along with appropriate dietary modifications and fluid input. Potassium citrate is often required to right thiazide-induced hypokalemia and hypocitraturia (see question 36). Chlorthalidone or indapamide may be substituted for hydrochlorothiazide for extra handy oncedaily dosing (see query 37). Thiazides are first-line remedy as a end result of they improve proximal (indirectly) and distal (directly) tubular reabsorption of calcium. However, thiazides could cause depletion of potassium and citrate, which ought to be changed with potassium citrate. If potassium supplementation is added, use amiloride with warning to avoid hyperkalemia. Additionally, indapamide is much less more probably to cause lipid disturbances related to the higher thiazide dosages wanted to reduce urinary calcium. About 10% to 20% of all kidney stones require surgical removing because of dimension and symptoms. Many urologists deal with symptomatic sufferers with calcium stones 1 to 2 cm in dimension in the renal pelvis or a big proximally obstructing stone (0. Each skilled has an opinion based on the expertise of the native medical group. Many asymptomatic stones can be monitored with out intervention aside from that noted in question 31. Specifics of stone location, duration, and general patient health are important in the decision. Other forms of lithotripsy embody percutaneous ultrasonic lithotripsy and endoscopic ultrasonic lithotripsy. Intracorporeal lithotripsy makes use of the holmium:yttrium-aluminum-garnet laser and electrohydraulic lithotripsy. Meschi T, Nouvenne A, Borghi L: Lifestyle suggestions to cut back the risk of kidney stones, Urol Clin N Am 38: 313�320, 2011. Pathogenesis, prognosis and administration, J Clin Endocrinol Metab 97:1847�1860, 2012.
110 mg sinemet visa
The administration of sufferers with drug-induced torsades consists of identifying and withdrawing the offending drugs treatment dynamics buy sinemet 110 mg online, replenishing the potassium stage to four symptoms in spanish sinemet 300 mg for sale. An interesting preventative strategy is by persistent therapy with the potassium-retaining aldosterone blocker, spironolactone. The danger of recurrences is markedly higher with metoprolol than with both propranolol or nadolol. Many patients be taught on their very own to abort episodes quickly after initiation with vagal maneuvers similar to gagging,Valsalva, or carotid massage. If the arrhythmia persists, sympathetic tone will increase and these maneuvers then become much less efficient. After intravenous administration, adenosine is cleared from the circulation inside seconds by mobile uptake and metabolism. Central administration ends in a more rapid onset of impact, and dosage discount is required. The really helpful adult dosage for peripheral intravenous infusion is 6 mg adopted by a second dose of 12 mg if essential. Most patients report transient dyspnea or chest pain after receiving a bolus of adenosine. However, the bradycardia usually resolves inside seconds and is changed with a mild sinus tachycardia. The beneficial initial dose of verapamil is 5 mg intravenously infused over 2 minutes. Diltiazem, 20 mg initially, followed by a second dose of 25 to 35 mg, is equally efficient. Atrial tachycardias may be because of a quantity of attainable mechanisms, and few information about acute pharmacologic termination of atrial tachycardias can be found. Atrial tachycardias associated to reentry around atriotomy scars are sometimes drug resistant, and their administration should resemble that of atrial flutter (see earlier in this chapter, p. If episodes produce solely minor symptoms and may be damaged easily by the affected person, persistent drug remedy may be averted. In circumstances by which recurrent episodes produce vital signs or require outside intervention for termination, both pharmacologic therapy or catheter ablation is acceptable. Patients with extensive atrial scarring, especially those with postoperative congenital coronary heart disease, could have multiple atrial arrhythmias and whole elimination of tachycardia in such sufferers remains challenging. Maze procedure (bottom right panel) involves a number of incisions of which only two are shown. Loss of atrial contraction, disturbed atrial endothelial operate, and activation of coagulation factor all predispose towards clot formation within the atria. Nonetheless, controlling irregular ventricular rates principally improves symptoms and train capability. Excess bradycardia could result in syncope or fatigue, whereas persistently faster rates could lead to a tachycardia-induced cardiomyopathy. Strict rate control is a resting coronary heart price lower than 80 beats per minute (bpm) and less than 110 bpm with minor exercise. The patients who were enrolled within the ratecontrol versus rhythm-control strategy trials cited beforehand have been thought-about candidates for both strategy. Intravenous therapy is often employed in patients who present acutely with extreme signs. The widespread pattern is slow-fast (middle panel), whereas fastslow conduction (bottom left panel) is unusual. For sufferers with extreme heart failure or marked hemodynamic instability, electrical cardioversion could additionally be required. Intravenous amiodarone can also be a pharmacologic option for fee management,122 with the added benefit that it may facilitate rhythm reversion. Quinidine was thought-about efficient, however received a lower rating because of potential toxicity. Intermittent drug self-administration must be used cautiously and solely in patients prone to tolerate this potential proarrhythmic impact. The efficacy of this approach is often examined in a monitored setting before being used on an outpatient foundation. Unfortunately, the effectiveness of obtainable antiarrhythmic agents is type of limited. In patients with no or minimal structural coronary heart disease, the first-line brokers are flecainide, propafenone, or sotalol. Dronedarone (see previous) has structural similarities to amiodarone and an identical antiarrhythmic profile. This drug choice algorithm is closely influenced by the potential for each drug to trigger proarrhythmia in susceptible people. Flecainide elevated mortality in patients with ischemic heart disease and propafenone probably has an identical impact. To translate this in to scientific practice requires outcomes of potential doubleblind trials, certainly one of which is testing the consequences of telmisartan. Atrial distention disturbs the atrial endothelium and activates hemostatic elements leading to a hypercoagulable state. Considering conventional remedy by warfarin, sufferers with a rating of 1 may be treated with both aspirin or warfarin. Protection of the brain has turn out to be the major focus of better management of embolization by the newer antithrombin and anti-Xa brokers. Canadian Cardiovascular Society Recommendations are that when oral anticoagulant remedy is indicated, the model new anticoagulants are preferable to warfarin for many sufferers. The main downside with all three medication is the danger of uncommon but doubtlessly deadly uncontrollable bleeding. No research in sufferers have yet assessed the power of prohemostatic medicine to antagonize excess anticoagulant results. Regardless of the relatively brief half-life of those brokers, instant reversal of the anticoagulant impact could additionally be wanted in case of major bleeding or emergency surgery. In these at intermediate threat, the net medical profit is particularly favorable with 316 8 - Antiarrhythmic Drugs and Strategies apixaban and both doses of dabigatran (110 mg and one hundred fifty mg twice daily). For these at low risk, apixaban and dabigatran 110 mg twice daily had a optimistic internet scientific profit. As comparative trials between these three brokers will probably by no means be done, this provisional modeling approach supplies extrapolations of clinical interest. The rivaroxaban group confirmed no difference from warfarintreated sufferers within the risk of main bleeding, but intracranial hemorrhage (0. Separate pointers for warfarin anticoagulation across the time of cardioversion have been 8 - Antiarrhythmic Drugs and Strategies 317 printed. If none is discovered, cardioversion could additionally be performed whereas anticoagulation is sustained. Even in sufferers with out danger components for stroke, anticoagulation is maintained for no less than four weeks after conversion. Atrial Flutter Traditionally, atrial flutter has been defined as an everyday atrial rhythm with a rate between 250 and 350 bpm within the absence of antiarrhythmic medicine.