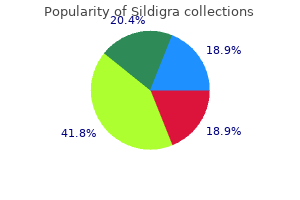
Discount 50 mg sildigra overnight delivery
A detailed understanding of airway anatomy is crucial for the anesthesia provider erectile dysfunction medicines order sildigra 50 mg overnight delivery. A full analysis of the airway and information of inauspicious airway predictors can alert the anesthesiologist to the potential for difficulty with airway management and allow for applicable planning erectile dysfunction doctor mumbai sildigra 25 mg order without a prescription. Apneic oxygenation can be used to delay the duration of apnea with out desaturation and is increasingly being adopted during the administration of each troublesome and routine airways. Application of local anesthesia to the airway or induction of common anesthesia is often required to facilitate airway management, to present consolation for the patient, and to blunt airway reflexes and the hemodynamic response to airway instrumentation. Tracheal intubation establishes a definitive airway, provides maximal safety towards aspiration of gastric contents, and permits for positive-pressure air flow with higher airway pressures than by way of a face masks or supraglottic airway. Flexible scope intubation of the trachea in an awake, spontaneously ventilating, and cooperative patient is the gold commonplace for the management of the tough airway. Invasive airways are indicated as a rescue approach when attempts at establishing a noninvasive airway fail. The anesthesia practitioner ought to turn out to be proficient with methods for transtracheal jet ventilation and cricothyrotomy. Extubation is a critical component of airway management with the potential for vital complications. The plan for extubation of the trachea should be preemptively formulated and includes a strategy for reintubation ought to the patient be unable to preserve an sufficient airway after extubation. Introduction General anesthesia is associated with numerous results on the respiratory system, including the lack of airway patency, lack of protecting airway reflexes, and hypoventilation or apnea. Therefore one of many elementary responsibilities of the anesthesiologist is to set up airway patency and to guarantee enough ventilation and oxygenation. The term airway management refers to the apply of creating and securing a patent airway and is a cornerstone of anesthetic practice. Because failure to safe a patent airway may end up in hypoxic brain harm or demise in only a few minutes, issue with airway administration has potentially grave implications. Poor assessment of the airway, poor planning, and a lack of non-public and/or institutional preparedness for managing difficulty with airway administration were the commonest contributing factors. As with any guide skill, continued practice improves performance and may scale back the likelihood of complications. New airway gadgets are regularly being launched into the clinical enviornment, every with distinctive properties that could be advantageous in sure conditions. The major variations in these algorithms are in particular particulars, such because the number of intubation attempts instructed, the specific alternate gadgets really helpful for troublesome intubation, and the organization of the algorithm. Nicholas Chrimes, a specialist anaesthetist in Melbourne, Australia, is one such cognitive aid designed to facilitate management of the unanticipated troublesome airway. If after an "optimal attempt" at each of those nonsurgical modalities alveolar oxygen delivery has not been achieved, then one "travels down the vortex," and an emergency surgical airway is indicated. Functional Airway Anatomy A detailed understanding of airway anatomy is important for the anesthesiologist. Assess the probability and scientific impact of basic administration problems: � Difficulty with affected person cooperation or consent � Difficult mask ventilation � Difficult supraglottic airway placement � Difficult laryngoscopy � Difficult intubation � Difficult surgical airway entry 2. Actively pursue alternatives to ship supplemental oxygen throughout the method of difficult airway management. Consider the relative deserves and feasibility of fundamental administration choices: � Awake intubation vs. Develop primary and various methods: Awake intubation Airway approached by noninvasive intubation Succeed* Fail Consider feasibility of different options(a) Invasive airway access(b)* Invasive airway access(b)* Intubation after induction of basic anesthesia Initial intubation makes an attempt successful* Initial intubation makes an attempt unsuccessful From this level onward, consider: 1. Therefore these options could additionally be of restricted value if this step within the algorithm has been reached through the Emergency Pathway. Invasive airway entry consists of surgical or percutaneous airway, jet ventilation, and retrograde intubation. Consider re-preparation of the affected person for awake intubation or cancelling surgery. Knowledge of normal anatomy and anatomic variations which will render airway management more difficult helps with the formulation of an airway management plan. Because some crucial anatomic buildings could additionally be obscured during airway management, the anesthesiologist must be familiar with the interrelationship between totally different airway constructions. The airway may be divided into the upper airway, which incorporates the nasal cavity, the oral cavity, the pharynx, and the larynx; and the lower airway, which consists of the tracheobronchial tree. The nasal cavity is divided into the best and left nasal passages (or fossae) by the nasal septum, which forms the medial wall of every passage. The septum is formed by the septal cartilage anteriorly and by two bones posteriorly- he ethmoid (superiorly) and the vomer (inferiorly). Nasal septal deviation is common within the adult population18; therefore the extra patent aspect must be determined before passing instrumentation through the nasal passages. The inferior meatus, between the inferior turbinate and the floor of the nasal cavity, is the preferred pathway for passage of nasal airway devices19; improper placement of objects within the nose may end up in avulsion of a turbinate. This fragile structure, if fractured, may end up in communication between the nasal and intracranial cavities and a resultant leakage of cerebrospinal fluid. Because the mucosal lining of the nasal cavity is very vascular, vasoconstrictor must be applied, often topically, earlier than instrumentation of the nostril to minimize epistaxis. The posterior openings of the nasal passages are the choanae, which lead into the nasopharynx. The hard palate, shaped by components of the maxilla and the palatine bone, makes up the anterior two thirds of the roof of the mouth; the taste bud (velum palatinum), a fibromuscular fold of tissue hooked up to the exhausting palate, forms the posterior one third of the roof of the mouth. The posterior wall of the pharynx is made up of the buccopharyngeal fascia, which separates the pharynx from the retropharyngeal house. Improper placement of a gastric or tracheal tube can outcome in laceration of this fascia and the formation of a retropharyngeal dissection. Along the superior and posterior walls of the nasopharynx are the adenoid tonsils, which may trigger continual nasal obstruction and, when enlarged, may cause problem passaging airway gadgets. The nasopharynx ends at the taste bud; this area is termed the velopharynx and is a typical site of airway obstruction in each awake and anesthetized patients. The base of the tongue lies in the anterior facet of the oropharynx, related to the epiglottis by the glossoepiglottic folds, which bound paired spaces known as the valleculae (although these are frequently referred to as a single area known as the vallecula). The area between the vocal cords is termed the glottis; the portion of the laryngeal cavity above the glottis is called the vestibule, and the portion inferior to the vocal cords is identified as the subglottis. It consists of 16 to 20 C-shaped cartilaginous rings that open posteriorly and are joined by fibroelastic tissue; the trachealis muscle varieties the posterior wall of the trachea. No single check has been devised to predict a difficult airway accurately 100 percent of the time; however, a whole evaluation of the airway and knowledge of the troublesome airway predictors can alert the anesthesiologist to the potential for problem and allow for appropriate planning. The cartilaginous framework of the larynx is made up of nine separate cartilages: the thyroid and cricoid cartilages; the paired arytenoid, corniculate, and cuneiform cartilages; and the epiglottis. The thyroid cartilage is the biggest of these cartilages and helps most of the soft tissues of the larynx. The arytenoid cartilages articulate with the posterior cricoid and are the posterior attachments for the vocal cords. The space inferior to the laryngeal inlet all the way down to the inferior border of the cricoid cartilage is the laryngeal cavity.
Buy sildigra 25 mg on line
Historically erectile dysfunction new treatments purchase sildigra 25 mg otc, such fistulae have typically been reported to be "rare erectile dysfunction medication covered by insurance sildigra 25 mg with amex," but the identification of such fistulae is a common echocardiographic discovering of which studies report a prevalence in the vary of 19% to 23% following myectomy. Though one study of 40 myectomy patients within the modern period discovered that nearly onequarter of such fistulae were nonetheless detectable by echocardiography at 6 months postoperatively. Less frequent diagnoses embody viral cardiomyopathy, postpartum cardiomyopathy, refractory valvular illness, primary myocardial diseases. The first commonest indication is idiopathic dilated cardiomyopathy, which accounted for roughly 46% of all cases in 2018. The selection standards have been broadened for each heart recipients and coronary heart donors. The method during which the donor heart is implanted has additionally changed, with a shift away from the basic biatrial approach (originally described by Lower and Shumway in 1960) to the bicaval Wythenshawe method described in the early Nineteen Nineties. In addition, this system has been demonstrated to be associated with shorter hospital stays. Furthermore, a number of sequence that compared the traditional Shumway approach with the bicaval approach confirmed larger 12-month survival in the bicaval group. Posttransplantation physiology, nevertheless, stays unchanged: the requisite denervation of the donor organ throughout harvesting leads to the absence of both direct afferent and efferent neural innervation via autonomic or somatic neural pathways after implantation. Significant dysrhythmias or arrhythmias in a transplanted coronary heart ought to be thought of harbingers of ischemia till proven otherwise. Developed in collaboration with the American Society of Echocardiography, Heart Rhythm Society, Angiography and Interventions and Society of Thoracic Surgeons. They could current for cardiac surgical procedure for the first time or for additional palliative correction, either definitively or for residua. Preoperative Anesthetic Considerations the distinctive issues of this inhabitants include the multisystem results of single-ventricle physiology, cyanosis, systemic proper ventricle, complicated intracardiac baffles, and failing subpulmonary proper ventricle. A full evaluation of each organ system is past the scope of this chapter, but readers are referred to the wonderful evaluate articles by Chassot and Bettex478 and by Lovell. One of the early scientific decisions to be made for an individual affected person entails figuring out the appropriateness of surgical care in a given institution. Preparation of the anesthetic plan requires detailed information of the anatomy and physiology of the lesion. Anesthetic concerns are lesion particular and are mentioned in several reviews. Elevated levels of erythropoietin in cyanotic patients can lead to a hyperviscosity syndrome and elevated danger of neurologic damage. Developed in collaboration with the American Society of Echocardiography, Heart Rhythm Society, Angiography and Interventions, and Society of Thoracic Surgeons. Shunt circulate may be influenced by changes in driving stress throughout a shunt or strain within the receiving chamber. The excessive intrathoracic strain that may happen with mechanical air flow, coughing, the Valsalva maneuver, bronchospasm, or positive end-expiratory stress can actually reverse the direction of a left-to-right shunt or no much less than make it bidirectional. Therefore, paradoxical embolization by clot or air is an actual risk in sufferers with intracardiac shunts and warrants fastidious attention to de-airing intravenous lines and careful administration of medicine by syringes by way of ports in intravenous strains. Shunts are generally labeled as restrictive or nonrestrictive in accordance with their blood velocity or strain traits measured at catheterization or by echocardiography. Large defects with related low-pressure gradients throughout them have nonrestrictive circulate. In addition, bigger defects could be anticipated to have a larger impact on downstream constructions and pressures. The mainstays of the anesthetic management of shunt lesions are understanding and controlling factors which will affect the direction and magnitude of the shunt. If the clinical problem is luxuriant pulmonary blood flow, a excessive Fio2 must be prevented. Similarly, the course and magnitude of the shunt flow determine whether or not one ought to hyperventilate a patient to achieve a low Paco2 or tolerate a high-normal Paco2. In the presence of a shunt, the potential dilation of the cardiac chambers and resultant enhance in chamber quantity and pressure are necessary. These conditions trigger hyperviscosity, which could be associated with hemostatic abnormalities. Many sufferers with congenital repairs that embrace a conduit or graft are maintained on antiplatelet medicines, and this ought to be noted. Intracardiac shunts are classically located at the level of the atria or ventricles. The magnitude of the shunt is often expressed by method of the ratio of pulmonary blood move (Qp) to systemic blood circulate (Qs): Qp/ Qs. A Qp/Qs ratio higher than 1 is mostly according to acyanotic heart disease and luxuriant pulmonary blood move. Intracardiac shunts and the Qp/ Qs are sometimes bidirectional, depending on situational physiology, and therefore should at all times be considered to be a threat for systemic embolization. Special point out of certain aortopulmonary shunts, used commonly prior to now to palliate some forms of cyanotic coronary heart disease, is warranted. The proximal connection could also be to the ascending aorta, brachiocephalic trunk, or subclavian artery. Because blood flow through this sort of shunt depends on systemic blood stress, systemic hypotension may lead to worsening hypoxemia. Furthermore, long-term publicity to these extracardiac shunts can outcome in left-sided chamber enlargement and dysfunction secondary to chronic volume overload. This is associated with exercise intolerance and decreased practical capability, which seem to have necessary prognostic implications. Regional anesthesia may be used for applicable procedures, but neuraxial blocks ought to be administered with caution due to the sympathetic blockade produced. Patients with important pulmonary hypertension are very sensitive to preload; subsequently, hypovolemia, ought to be handled instantly and aggressively. As in adult patients with acquired heart disease, the presence of ventricular dysfunction is an important risk factor for morbidity and mortality, both in the perioperative interval and in the long term. Additionally, atrial fibrillation causes 24% of strokes in sufferers older than 80 years old. The transition of the electrical signal from one type of tissue to the other is probably liable for this arrhythmia. The classic Maze process is at present the most effective curative remedy for atrial fibrillation. A commercially available bipolar instrument allows the operator to assess transmurality. Currently, newer applied sciences allow the speedy creation of traces of conduction blockade, which surgeons use to ablate atrial fibrillation in sufferers undergoing concomitant cardiac surgical procedures. These technologies include alternate vitality sources corresponding to radiofrequency and microwave power, ultrasound, cryotherapy, and laser (Table 54. These applied sciences are additionally used in minimally invasive surgical ablation procedures to cure isolated atrial fibrillation.

Sildigra 100 mg purchase with amex
Chronically opioid-consuming patients want their day by day systemic dosage by the intravenous or oral path to erectile dysfunction young adults treatment order 50 mg sildigra fast delivery forestall withdrawal erectile dysfunction protocol pdf buy sildigra 100 mg fast delivery. Remove opioid patch when main surgery is deliberate; in minor surgery patch could additionally be continued with out background infusion. Every continual pain affected person has to be seen postoperatively tid to consider ache at relaxation, ache with exercise. Change strategy of postoperative analgesia if inadequate use persists despite repeated patient education. Reduce day by day opioid doses after the second postoperative day stepwise to the preexisting dose. When switching back to transdermal route consider 12-16 h delayed results and provide patient for this period with sufficient on-demand analgesia. Do not attempt to clear up a chronic ache downside in the immediate postoperative interval. Use non-pharmacological techniques (distraction, relaxation) where applicable and offer counselling within the ache unit after postoperative restoration. Opioids from immunocytes work together with receptors on sensory nerves to inhibit nociception in inflammation. Modulation of peripheral sensory neurons by the immune system: implications for pain therapy. Mycobacteria attenuate nociceptive responses by formyl peptide receptor triggered opioid peptide launch from neutrophils. Beta-endorphin, Metenkephalin and corresponding opioid receptors within synovium of sufferers with joint trauma, osteoarthritis and rheumatoid arthritis. Involvement of intraarticular corticotropin-releasing hormone in postoperative ache modulation. Arthritic irritation in rats as a mannequin of continual ache: role of opioid systems. Codeine and opioid metabolism: implications and alternate options for pediatric ache administration. Analgesia and opioids: a pharmacogenetics shortlist for implementation in clinical apply. Practice tips for persistent ache management: an updated report by the American Society of Anesthesiologists task drive on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine. Chronic ailments in the European Union: the prevalence and well being cost implications of persistent ache. Risk factors for ulcerative oral mucositis in most cancers sufferers: unanswered questions. Multimodal pain therapy in persistent noncancer pain-gold standard or need for further clarification The role of the health insurance trade in perpetuating suboptimal ache administration. Evidence-based scientific knowledge documenting the treatment and cost-effectiveness of complete pain packages for continual nonmalignant ache. Beyond the needle: expanding the position of anesthesiologists in the management of continual non-malignant pain. Acceptance and values-based motion in continual ache: a three-year follow-up evaluation of therapy effectiveness and course of. Systematic review to decide which validated measurement tools can be used to assess danger of problematic analgesic use in sufferers with chronic ache. Multidisciplinary biopsychosocial rehabilitation for continual low back pain: Cochrane systematic review and meta-analysis. Improved high quality of life, working capacity, and affected person satisfaction after a pretreatment multimodal evaluation technique in patients with combined chronic muscular pain: a randomized-controlled examine. Physical conditioning applications for bettering work outcomes in employees with back pain. Placebo analgesia and past: a melting pot of concepts and concepts for neuroscience. Regulation of mu-opioid receptors: desensitization, phosphorylation, internalization, and tolerance. Pain inhibition by blocking leukocytic and neuronal opioid peptidases in peripheral infected tissue. Progress in understanding mechanisms of opioid-induced gastrointestinal opposed results and respiratory depression. Opioid unwanted effects and their treatment in patients with persistent cancer and noncancer pain. Immunosuppressive features of analgesics and sedatives used in mechanically ventilated sufferers: an underappreciated danger issue for the event of ventilator-associated pneumonia in critically unwell sufferers. Precipitated opioid withdrawal throughout acute bodily dependence induction methods. Perioperative and intraoperative pain and anesthetic care of the persistent pain and most cancers pain affected person receiving continual opioid therapy. MorphiDex (morphine sulfate/dextromethorphan hydrobromide combination) within the remedy of persistent pain: three multicenter, randomized, doubleblind, controlled clinical trials fail to show enhanced opioid analgesia or reduction in tolerance. Defining clinical issues around tolerance, hyperalgesia, and dependancy: a quantitative and qualitative consequence examine of long-term opioid dosing in a chronic pain follow. Opioid withdrawal will increase transient receptor potential vanilloid 1 activity in a protein kinase A-dependent manner. Gradual withdrawal of remifentanil infusion may stop opioidinduced hyperalgesia. Strategies for making analgesia safer: the role of comparative effectiveness research. Side effects related to current and prospective antimigraine pharmacotherapies. Pharmacotherapy for neuropathic ache in adults: a scientific evaluation and meta-analysis. Topical analgesics for acute and persistent ache in adults - an outline of Cochrane Reviews. How are topical opioids used to manage painful cutaneous lesions in palliative care Inflammation of the rat paw enhances axonal transport of opioid receptors in the sciatic nerve and increases their density within the infected tissue. Painful inflammation-induced improve in mu-opioid receptor binding and G-protein coupling in major afferent neurons. Modulation of tight junction proteins in the perineurium to facilitate peripheral opioid analgesia. Analgesic efficacy of peripheral opioids (all besides intra-articular): a qualitative systematic review of randomised managed trials. Leukocyte opioid receptors mediate analgesia by way of Ca(2+)-regulated launch of opioid peptides. Single-dose intra-articular morphine after arthroscopic knee surgical procedure: a meta-analysis of randomized placebo-controlled studies.
| Comparative prices of Sildigra |
| # | Retailer | Average price |
| 1 | OSI Restaurant Partners | 739 |
| 2 | Dillard's | 386 |
| 3 | Delhaize America | 588 |
| 4 | Walgreen | 763 |
| 5 | Rite Aid | 637 |
Sildigra 25 mg amex
Indwelling intercostal catheters are an choice however they are often troublesome to position reliably percutaneously impotence at 55 buy discount sildigra 25 mg on line. It is important to avoid injection into the intercostal vessels erectile dysfunction caused by low testosterone 25 mg sildigra cheap overnight delivery, that are adjoining to the nerve in the intercostal groove. It can be important to place the block close to the posterior axillary line to be certain to block the lateral cutaneous branch of the intercostal nerve. Liposomal encapsulated bupivacaine has a gradual release of local anesthetic over a interval of 72 to ninety six hours. In combination with multimodal techniques, the postoperative analgesia could also be corresponding to thoracic epidural analgesia. Spinal injection of opioids can have a period of analgesia that approaches 24 hours after thoracotomy. Because of the concerns of possible infection with subarachnoid catheters and the need to repeat spinal injections, investigation and remedy has focused on epidural techniques. A meta-analysis of respiratory problems after varied forms of surgical procedure has shown that epidural methods scale back the incidence of respiratory complications. Opioid and native anesthetic combinations present better analgesia at lower doses than both drug alone. Ultrasound steerage has not but confirmed to be as useful for thoracic epidural catheter placement as it has for different kinds of regional blockade. After injection of a small volume of saline (5 mL) via the Tuohy needle, the epidural pressure may be transduced and a typical waveform could be seen that identifies the epidural house with a excessive diploma of sensitivity and specificity. The needle is inserted 1 cm lateral to the superior tip of the spinous course of and then superior perpendicular to all planes to contact the lamina of the vertebral body immediately beneath. The needle is then "walked" up the lamina at an angle rostrally (45 degrees) and medially (20 degrees) until the rostral fringe of the lamina is felt. The needle is then superior over the sting of the lamina in search of a loss of resistance on getting into the epidural space after transversing the ligamentum flavum. The needle is inserted next to the rostral fringe of the spinous process and superior straight with none angle from the midline. Philadelphia: Saunders; 1996) Research has make clear the pharmacology, which underlies the synergy between native anesthetics and opioids to produce segmental epidural analgesia. In a double-blind randomized study, Hansdottir and associates345 in contrast epidural infusions of lumbar sufentanil, thoracic sufentanil, and thoracic sufentanil plus bupivacaine (S+B) for postthoracotomy analgesia. Thoracic sufentanil plus bupivacaine offered considerably better analgesia with motion and less sedation than the opposite infusions. Although sufentanil dosages and serum ranges have been significantly decrease within the mixed (S+B) group than within the other two groups, lumbar cerebral spinal fluid levels of sufentanil at 24 and 48 hours had been larger in the mixed group than in the thoracic sufentanil group (this means that the native anesthetic facilitates entry of the opioid from the epidural space into the cerebral spinal fluid). Differences in lipid solubility that create comparatively minor clinical differences in the results of opioids when used systemically cause main variations in the effects of those identical opioids when used neuraxially. However, these lipid-soluble agents have important absorption and systemic results when used as epidural infusions. A catheter can be positioned within the thoracic paravertebral area both percutaneously or by approaching the space anteriorly and directly when the chest is open intraoperatively. Saline is injected via the Tuohy needle to hydrodissect the paravertebral space and an epidural catheter is handed into the pocket that has been created within the paravertebral area and then secured at the skin. Paravertebral local anesthetics present a dependable multilevel intercostal blockade that tends to be unilateral with a low tendency to unfold to the epidural house. It has not yet been demonstrated if paravertebral analgesia can contribute to a decrease in respiratory morbidity in high-risk cases, which has been shown for thoracic epidural analgesia. The serratus anterior aircraft block is performed on the degree of the fifth rib in the midaxillary line. At this degree, the serratus anterior muscle may be identified overlying the ribs, with the latissimus dorsi muscle lying superior to the serratus muscle. Needle insertion can be performed in-plane or out-of-plane, relying on provider choice. The serratus anterior plane block may be achieved by injecting native anesthetic either above or beneath the serratus muscle, with equal analgesic unfold with both techniques. Serratus anterior aircraft block has been proven to improve the analgesia offered by patient-controlled morphine. The space is certain medially by the vertebral body, posteriorly by the costotransverse ligaments and the heads of the ribs, and anteriorly by the endothoracic fascia and parietal pleura. A catheter is then handed 5 cm distal to the tip of the needle and an infusion of 5 to 8 mL/h is begun. This suggests that chronic pain after thoracic surgical procedure may be partially preventable by intensive administration of acute postoperative ache. Patients may be utilizing physician prescribed opioids for pain related to their thoracic pathology, or different persistent pain syndromes. Active abusers of narcotics or those in a rehabilitation program receiving day by day methadone are also included on this group. Whenever possible, sufferers should take their common analgesia or methadone preoperatively; in any other case substitute opioids must be provided. The opioid doses required to produce adequate postoperative analgesia are elevated. A choice should be made relating to the strategy of elevated opioid supply, both systemically and/or via an epidural. An elevated narcotic dose may be supplied within the epidural solution, or standard narcotic concentrations could also be used in the epidural with extra systemic narcotic. More frequently, the affected person receives a standard or barely increased focus of opioid within the epidural infusion and extra systemic opioid to minimize the prevalence of withdrawal. A handy way to provide drug supply in patients not immediately in a position to take oral treatment is within the type of a transdermal fentanyl patch. Systemic opioids may be offered as a steady intravenous infusion or in oral format. By postoperative day 4, 32% of sufferers had shoulder ache, however only 7% had clinically relevant shoulder ache. This is thought to originate from phrenic nerve afferent fibers and associated to diaphragmatic or mediastinal irritation. This pain was associated with tenderness of the involved shoulder muscular tissues and ache with movement. Of the two types, the musculoskeletal pain was extra intense and more difficult to deal with. The block needle (dotted arrow) is advanced in a cranial-caudal course to contact the transverse course of. Patient-controlled analgesic methods are often tough to manage in these patients and so they could additionally be finest managed with fastened dosage regimens that are modified as needed. Ultimately, after dose titration the patient may be receiving each increased epidural opioid and greater than preoperative doses of systemic opioid, without vital unwanted effects. Patients in whom epidural bupivacaine-morphine analgesia is inadequate could respond to a change to bupivacainesufentanil. They regularly can take their full methadone dose all through the perioperative interval.
Order 25 mg sildigra fast delivery
Solitary B lines are a normal finding in the regular lung erectile dysfunction medscape 120 mg sildigra order free shipping, and elevated numbers are observed in disease erectile dysfunction causes alcohol 50 mg sildigra purchase visa. Ultrasonography findings for pneumothorax are the absence of lung sliding, B traces, and lung pulse, and the presence of lung points. The presence of echogenic materials within the effusion suggests an exudate or hemorrhage, although some exudates are anechoic. The M-mode ultrasound scan shows parallel lines indicative of no shifting structure underlying the probe. The ultrasonographic finding designated as a lung point is discovered in the presence of pneumothorax and represents the imaging of the cyclic transition throughout respiratory from the absence of any sliding or moving B traces at a bodily location. Lung consolidations may be attributable to an infection, pulmonary embolism, lung cancer and metastasis, compression atelectasis, obstructive atelectasis, and lung contusion. Additional sonographic signs that will assist decide the purpose for lung consolidation include the quality of the deep margins of the consolidation, the presence of comet-tail reverberation artifacts on the far-field margin, the presence of air or fluid bronchograms, and the vascular sample throughout the consolidation. The methodology is clinically available and has reasonable to low spatial resolution but excessive temporal resolution, thus permitting for assessment of regional ventilation in real-time. High concentrations of electrolytes, extracellular water content material, large cells, and number of cell connections by gap junctions as current in blood and muscular tissues reduce impedance. During the respiratory cycle, thoracic bioimpedance is influenced basically by each air flow and perfusion. The location is chosen based mostly on the medical information desired, normally at the fifth intercostal space for traditional lung evaluation. Direct assessment of lung circumstances could be accomplished by evaluating low impedance. For capillary blood samples obtained from finger and ear punctures, a significant correlation exists between optical-based and automatic laboratory Hb analysis, with a nonsignificant bias. Fingerstick samples might approximate commonplace laboratory Hb measurements higher than earlobe samples. This is a known reason for inaccurate blood fuel measurements and occurs when PaO2 is decreased by increased O2 consumption as a end result of markedly elevated white blood cell counts within the arterial blood pattern. Measurement error is further aggravated by delayed laboratory evaluation or incorrect sampling. Pseudohypoxemia happens not only in hyperleukocytosis but also in thrombocytosis associated with polycythemia vera. Specific issues for respiratory monitoring in particular conditions are detailed in the subsequent part. These gadgets could also be either pressure or time cycled, and each the mean airway strain and oscillatory stress amplitude are displayed on the console to the clinician. During typical mechanical air flow, airway strain and flow are associated in accordance with basic mechanical properties of the respiratory system, similar to airway resistance and tissue compliance. During rigid bronchoscopy or laryngeal interventions, the anesthesiologist is required to share administration of the airway with the surgeon. Analysis of arterial blood gasoline measurements should be carried out inside 30 minutes of any change in ventilator settings, and a minimum of twice per day on steady settings. Recent studies counsel that oscillation using a number of simultaneous frequencies may improve the effectivity of fuel trade, reduce the heterogeneity of parenchymal strain, and preserve lung recruitment at lower imply airway pressures. This jet of gasoline, together with entrained air from the surrounding setting, leads to insufflation of the lungs. The complete system is open to the environment, thus resulting in important escape of respiratory gases. Gas could be sampled at the distal finish of the catheter or rigid bronchoscope by way of a dedicated channel. Transport of adult and pediatric sufferers from areas with superior monitoring to extra distant locations is fraught with issue, starting from easy gear malfunction to major disasters. The lack of standardized monitoring techniques and terminology explains the broadly reported discrepancies in the incidence of adverse events. Overall, a excessive incidence of respiratory issues following transport has been reported. If a transport ventilator is used, airway pressures ought to be available in numeric or graphic forty one � Respiratory Monitoring 1333 codecs. Human elements are essential during transport, and a specialized transport group using standardized management procedures with preparatory, switch, and posttransport stabilization phases doubtless limits the frequency of adverse events. Adequate O2 supply with functioning low-pressure alarms must be verified throughout pretransport preparation. Nitrogen washout methods are present in commercial mechanical ventilators for intensive care use. Such techniques provide data from medical devices, clinical data management techniques, and laboratory data. The availability of huge quantities of real-time data in digital type permits for introduction of recent approaches to monitoring which will have been conceptualized, however not but clinically implemented. Humans are restricted in their capability to analyze large portions of knowledge precisely and repeatedly. Accordingly, computer algorithms that identify delicate however meaningful tendencies in physiologic data are fascinating. Such instruments require relevant contextualization of measurement to enhance accuracy, in addition to minimization of false-negative and false-positive alarms. This automated monitoring should depend not only on well timed measurements, but also on prior info. Algorithms with established clinical guidelines provide the chance to detect subtle changes in time-series information,383 which exceed human discrimination. Some instruments of respiratory monitoring have been assessed in adult and pediatric populations. Such automated methods allow for the implementation of extra ranges of safety. Expeditious evaluation of circulating blood gases could facilitate sooner initiation of required remedy and adjustment of implemented air flow. These measurements have been helpful in intensive care administration of neonates and infants,393 and in the fields of wound therapeutic and hyperbaric O2 remedy. O2 transducers are electrochemical polarographic Clark-type electrodes by which the speed of chemical response is said to an electrical sign proportional to the O2 concentration. The skinny epidermal layer of infants facilitates the measurements, in distinction to the diffusion barrier launched by the thicker adult pores and skin. However, in very preterm infants, monitoring at 40�C or 41�C to scale back the danger of burns is feasible, supplied a bias correction of 12% to 15% is utilized. In sufferers present process noninvasive ventilation, unacceptably extensive variability may be observed. PtcO2 from regular to extraordinarily low-birth-weight infants agreed well with PaO2 measurements, with imply PtcO2-PaO2 difference 2. The use of PtcO2 in adults has been focused on wound management, peripheral vascular illness, and hyperbaric medicine. Although attempts for purposes in adults have been promising, similar to the utilization of PtcO2 to help resuscitative efforts,402 measurements following off-pump coronary artery surgical procedures still current very excessive variability.
Sildigra 50 mg generic free shipping
The main effect of catecholamines on the splanchnic capacitance vessels is venoconstriction erectile dysfunction pills pictures sildigra 120 mg cheap with amex, which actively forces out splanchnic blood erectile dysfunction condom purchase sildigra 120 mg on-line, reduces splanchnic venous capacitance, and increases venous return to the center. Compliant regions (dashed lines) of the higher and decrease a half of the body and end-diastolic volumes of the left ventricle in control state (left panel) are proven after occlusion of the aorta alone (middle panel) and mixed occlusion of the aorta and inferior vena cava (right panel). Cross-clamping the thoracic aorta in canine leads to marked will increase in mean arterial stress and end-diastolic left ventricular stress (84% and 188%, respectively) and no significant change in stroke quantity. By transfusing blood (above the clamps) throughout this era of simultaneous clamping, the authors reproduced the hemodynamic effect of thoracic aortic cross-clamping alone. This research also demonstrated that thoracic aortic cross-clamping is associated with a big and dramatic improve (155%) in blood move above the level of the clamp whereas no change in blood move occurred with simultaneous aortic and inferior vena cava clamping. These experimental information strongly help the speculation of blood volume redistribution during aortic cross-clamping and help clarify the marked variations in hemodynamic responses observed after aortic cross-clamping at different levels. The impaired left ventricle could respond to increased afterload with a rise in end-systolic volume and a concomitant discount in stroke quantity (afterload mismatch). The reduction in stroke volume could additionally be due to restricted preload reserve, myocardial ischemia, or lack of ability of the guts to generate a pressure-induced increase in contractility (the Anrep effect). If proper ventricular function stays normal, the pre-clamp right ventricular stroke quantity added to the elevated left ventricular end-systolic quantity ends in left ventricular dilation and elevated end-diastolic quantity. Most medical research indicate that cardiac output decreases with thoracic aortic cross-clamping (without vasodilator therapy or diverting circulatory support), whereas most animal research show no important change or a rise in cardiac output. Whereas a normal intact heart can face up to large will increase in quantity without significant ventricular distention or dysfunction, an impaired coronary heart with decreased myocardial contractility and coronary reserve may reply to such improve in volume situations with marked ventricular distention because of acute left ventricular dysfunction and myocardial ischemia. Although impaired myocardial contractility and decreased coronary reserve are uncommon in animal experiments, such problems are frequent within the aged population undergoing aortic reconstruction. The enhance in ventricular loading circumstances seen with thoracic and supraceliac cross-clamping55,fifty six within the scientific setting may increase left ventricular wall stress (afterload), with resultant acute deterioration of left ventricular operate and myocardial ischemia. Impaired subendocardial perfusion brought on by excessive intramyocardial pressure may be the purpose for wall motion abnormalities and changes in ejection fraction. Reflex mechanisms inflicting instant suggestions inhibition may also clarify the reduction in cardiac output with aortic cross-clamping. For instance, baroreceptor activation resulting from elevated aortic pressure ought to depress the guts fee, contractility, fifty six � Anesthesia for Vascular Surgery 1835 and vascular tone. Thoracic aortic cross-clamping with the utilization of vasodilator remedy to normalize ventricular loading situations maintains or increases cardiac output. Cross-clamping of the thoracic aorta decreases total-body O2 consumption by approximately 50%. For reasons that are unclear, O2 consumption decreases in tissues above the clamp. In clinical research, elevated mixed venous O2 saturation happens with aortic cross-clamping above the celiac axis. This improve in blended venous O2 saturation could also be explained by a discount in O2 consumption that exceeds the reduction in cardiac output, thus reducing whole body O2 extraction. Central hypervolemia and increased arteriovenous shunting in tissues proximal to the aortic clamp could play a task in reducing whole body O2 extraction. Arterial blood stress, blood move, and O2 consumption distal to a thoracic aortic cross-clamp lower by 78% to 88%, 79% to 88%, and 62%, respectively, from baseline values before clamping. Blood circulate through tissues and organs under the extent of aortic occlusion is dependent on perfusion strain and is impartial of cardiac output. Administration of sodium nitroprusside to keep proximal aortic strain above the cross-clamp at pre-clamp levels has been proven to further cut back arterial stress distal to the clamp by 53%. As mentioned later, these information have vital implications relating to important organ safety throughout aortic cross-clamping. The cardiovascular response to infrarenal aortic crossclamping is much less vital than with high aortic crossclamping (see Table fifty six. Although a number of scientific reports have noted no significant hemodynamic response to infrarenal cross-clamping, the hemodynamic response generally consists of will increase in arterial strain (7% to 10%) and systemic vascular resistance (20% to 32%), with no vital change in heart rate. In this example, blood quantity below the clamp shifts to the compliant venous segments of the splanchnic circulation above the clamp, thereby dampening the anticipated enhance in preload. The preload modifications with infrarenal aortic cross-clamping also could depend upon the status of the coronary circulation. Echocardiographically detected segmental wall movement abnormalities happen in as a lot as 30% of patients throughout infrarenal aortic reconstruction, with over 60% occurring on the time of aortic cross-clamping. Acute renal failure happens in roughly 3% of patients undergoing elective infrarenal aortic reconstruction, and mortality ensuing from postoperative acute renal failure is extra frequent than 40%. Despite important enhancements in the perioperative care of those sufferers, the frequent incidence of morbidity and mortality resulting from acute renal failure has remained largely unchanged over the last several decades. Most of the morbidity related to significant postoperative renal dysfunction is nonrenal. Procedures requiring aortic cross-clamping above the renal arteries dramatically scale back renal blood circulate. Experimental research report an 83% to 90% reduction in renal blood flow during thoracic aortic cross-clamping. Infrarenal aortic cross-clamping in humans is associated with a 75% increase in renal vascular resistance, a 38% lower in renal blood flow, and a redistribution of intrarenal blood circulate towards the renal cortex. These quite profound alterations in renal hemodynamics occurred despite no important change in systemic hemodynamics, and they persisted after unclamping. The sustained deterioration in renal perfusion and performance throughout and after infrarenal aortic cross-clamping has been attributed to renal vasoconstriction, however the specific pathophysiologic course of stays unknown. Other mediators, corresponding to plasma endothelin, myoglobin, and prostaglandins, might contribute to the decreased renal perfusion and function after aortic cross-clamping. Acute tubular necrosis accounts for almost all the renal dysfunction and failure after aortic reconstruction. The diploma of preoperative renal insufficiency stays the strongest predictor of postoperative renal dysfunction. In addition to aortic cross-clamping-induced reductions in renal blood flow, ischemic reperfusion damage, intravascular quantity depletion, embolization of atherosclerotic debris to the kidneys, and surgical trauma to the renal arteries all contribute to renal dysfunction. Mannitol, loop diuretics, and dopamine are used clinically to preserve renal perform throughout aortic surgical procedure. Significant controversy exists relating to the usage of these drugs, in addition to the mechanisms by which they might provide a protecting impact. Although not proved, pharmacologic "protection" earlier than aortic cross-clamping is believed to be beneficial and is therefore given. Mannitol improves renal cortical blood circulate during infrarenal aortic cross-clamping and reduces ischemia-induced renal vascular endothelial cell edema and vascular congestion. Other mechanisms by which mannitol may be useful include performing as a scavenger of free radicals, lowering renin secretion, and increasing renal prostaglandin synthesis. Routine use of these medication is common for patients with preoperative renal insufficiency and for procedures requiring suprarenal aortic cross-clamping.
Discount sildigra 100 mg without a prescription
Rational therapeutic strategies to prevent the deleterious effect of aortic cross-clamping primarily embrace measures to scale back afterload and maintain a standard preload and cardiac output erectile dysfunction treatment south africa buy discount sildigra 100 mg. Vasodilators erectile dysfunction drugs for diabetes sildigra 25 mg purchase free shipping, positive and negative inotropic drugs, and controlled intravascular volume depletion. Patients with impaired ventricular function requiring supraceliac aortic cross-clamping are the most difficult. Myocardial ischemia, reflecting an unfavorable steadiness between myocardial O2 provide and demand, might outcome from the hemodynamic penalties of aortic crossclamping. Afterload discount, mostly completed with using sodium nitroprusside or clevidipine (predominantly arteriolar dilators), is critical to unload the guts and scale back ventricular wall rigidity. In a large collection of patients requiring cross-clamping of the descending thoracic aorta, stable left ventricular function was maintained with sodium nitroprusside throughout cross-clamping. Sodium nitroprusside most likely allowed adequate intravascular quantity earlier than unclamping, which resulted in steady unclamping hemodynamics. Nitroglycerin can be utilized as a result of it increases venous capacity more than does sodium nitroprusside. In sufferers with out evidence of left ventricular decompensation or myocardial ischemia during supraceliac aortic cross-clamping, a proximal aortic mean arterial pressure of up to a hundred and twenty mm Hg is suitable. The surgeon might request decrease proximal arterial strain if friable aortic tissue is encountered. Blood circulate beneath the aortic clamp is dependent upon pressure and decreases additional during therapy with vasodilators. In this setting, vital organs and tissues distal to the clamp are uncovered to lowered perfusion stress and blood circulate. Though rare, maintenance of enough cardiac output may require lively intervention with inotropic medication. The hemodynamic response to unclamping is determined by many components, including the extent of aortic occlusion, whole occlusion time, use of diverting support, and intravascular volume. Reactive hyperemia in tissues and organs distal to the clamp and the resultant relative central hypovolemia are the dominant mechanisms of the hypotension. AoX, Aortic cross-clamping; Cven, venous capacitance; R art, arterial resistance; Rpv, pulmonary vascular resistance. These humoral elements and mediators, which may also play a task in organ dysfunction after aortic occlusion, include lactic acid, renin-angiotensin, O2 free radicals, prostaglandins, neutrophils, activated complement, cytokines, and myocardial-depressant components. It is crucial that correction of preoperative fluid deficits, upkeep of intraoperative fluid requirements, and alternative of blood loss be accomplished before unclamping. Vasodilators, if used, should be steadily reduced and discontinued before unclamping. Moderate augmenting of intravascular quantity by administration of fluids (500 mL) in the course of the immediate prerelease interval is indicated for infrarenal unclamping. More aggressive intravascular fluid administration is required in the period instantly previous supraceliac unclamping. If vital hypotension results, gradual release of the aortic clamp and reapplication or digital compression are necessary measures in maintaining hemodynamic stability throughout unclamping. Although vasopressor necessities are minimal after release of the infrarenal clamp, important assist is commonly needed after the removing of supraceliac clamps. Caution should be noticed when vasopressor assist is used in this setting because profound proximal hypertension could happen if reapplication of the cross-clamp is required above the celiac axis. In addition, hypertension ought to be prevented to forestall damage to or bleeding from the vascular anastomoses. The alternative of the type and the dimensions of the central line could be decided on a case-by-case basis. Placement of an arterial catheter must be routine in all sufferers undergoing aortic reconstruction. A noninvasive blood pressure cuff must be placed on the arm contralateral to the arterial catheter within the event of catheter malfunction. It should be reserved for patients with severely restricted cardiopulmonary function or complicated aortic reconstruction. The invasive monitoring catheters could be placed earlier than or after induction of general anesthesia. With selective use, correct interpretation of knowledge, and rational remedy methods, pulmonary artery catheter monitoring could also be useful in high-risk patients present process complicated aortic reconstruction. Yet the clinical value of pulmonary artery catheter monitoring in high-risk sufferers has not been established. The scientific usefulness of any monitoring method in the end is dependent upon affected person choice, correct interpretation of knowledge, and acceptable therapeutic intervention. The routine use of cell salvage during aortic surgery may not be cost-effective and thus it may best be reserved for a select group of patients with an anticipated giant blood loss. A costeffective choice is to use the cell salvage reservoir for blood assortment and activate the total salvage course of provided that giant blood loss happens. Cell Salvage Intraoperative cell salvage is a widely used method mixed with allogenic blood transfusion and in some facilities is considered routine. An early, nonrandomized examine reported a 75% discount in the number Anesthetic Drugs and Techniques Various anesthetic techniques, together with basic anesthesia, regional (epidural) anesthesia, and mixed methods, have been used efficiently for belly aortic reconstruction. Combined methods mostly use a lumbar or low thoracic epidural catheter in addition to common anesthetic. Local anesthetics, opioids, or, extra commonly, a combination of the two may be administered by bolus or continuous epidural infusion. Maintenance of significant organ perfusion and function by the provision of secure perioperative hemodynamics is more important to total consequence than is the selection of anesthetic drug or approach. Given the frequent incidence of cardiac morbidity and mortality in sufferers present process aortic reconstruction, factors that influence ventricular work and myocardial perfusion are of prime importance. Induction of basic anesthesia should ensure that steady hemodynamics are maintained throughout loss of consciousness, laryngoscopy and endotracheal intubation, and the quick postinduction period. The addition of a short-acting, potent opioid similar to fentanyl or sufentanil normally offers stable hemodynamics during and after induction of anesthesia. Volatile anesthetics could also be administered in low concentrations earlier than endotracheal intubation throughout assisted ventilation as an adjunct to blunt the hyperdynamic response to laryngoscopy and endotracheal intubation. Esmolol 10 to 25 mg, sodium nitroprusside 5 to 25 g, nitroglycerin 50 to one hundred g, or clevidipine one hundred mcg and phenylephrine 50 to a hundred g must be obtainable for bolus administration throughout induction if wanted to maintain acceptable hemodynamics. Maintenance of anesthesia could additionally be completed with a mix of a potent opioid (fentanyl or sufentanil) and an inhaled anesthetic (sevoflurane, desflurane, or isoflurane). Patients with extreme left ventricular dysfunction could benefit from a pure opioid method, but a balanced anesthetic technique permits the clinician to take benefit of probably the most desirable traits of potent opioids and inhaled volatile anesthetics while minimizing their undesirable unwanted side effects. Nitrous oxide can be utilized to complement either an opioid or an inhaled anesthetic. Various regional anesthetic and analgesic methods have been used successfully throughout and after aortic reconstruction. For over 2 a long time, interest has focused on the usage of regional anesthetic and analgesic techniques to scale back the incidence of perioperative morbidity in patients undergoing aortic reconstruction. The benefits of combined fifty six � Anesthesia for Vascular Surgery 1839 basic and epidural anesthesia intraoperatively, with or without epidural analgesia continued into the postoperative interval, remain controversial.
Sildigra 50 mg online buy cheap
Although this feature typically leads to superb postoperative ache relief erectile dysfunction 70 year olds sildigra 120 mg generic without a prescription, it could be undesirable in some patients due to the possible danger of nerve or tissue injury in a partially blocked limb erectile dysfunction pump demonstration buy 120 mg sildigra otc. A short- or medium-acting local anesthetic, such as lidocaine or mepivacaine, may be extra acceptable for surgical anesthesia. Whatever drug is chosen, the whole dosage must be calculated for each patient and must be saved within safe limits (see Chapter 29 for details). Vasoconstrictors, often epinephrine, may be added to the chosen local anesthetic to enhance onset of action, to lower drug uptake, and to prolong action. Ideally, the epinephrine ought to be added to the native anesthetic at the time the block is to be carried out. Complications and Safety Nerve injury is a recognized complication of peripheral regional techniques (Box forty six. Risk factors contributing to neurologic deficit after regional anesthesia embody neural ischemia, traumatic damage to the nerves during needle or catheter placement, and an infection. However, postoperative neurologic harm due to pressure from improper affected person positioning, tightly applied casts or surgical dressings, and surgical trauma is commonly attributed to the regional anesthetic. Patient factors corresponding to body habitus or a preexisting neurologic dysfunction can even contribute. Theoretically, localization of neural buildings with a nerve stimulator or ultrasound guidance would allow a high success fee with out increasing the risk of neurologic problems, but this has not been established. These sonograms have been obtained in the axilla earlier than (A) and after (B) injection in the musculocutaneous nerve. Nerve expansion is detected but with preservation of the general integrity of the nerve borders. In laboratory fashions, the addition of epinephrine will increase the neurotoxicity of local anesthetic solutions and decreases nerve blood move; nevertheless, the scientific relevance of these findings in people stays unclear. Nerve damage attributable to traumatic needle placement, local anesthetic neurotoxicity, and neural ischemia through the efficiency of a regional anesthetic can worsen neurologic consequence within the presence of an additional affected person factor or surgical damage. Hemorrhagic issues have been described with practically each peripheral technique and vary from localized bruising and tenderness to severe hematomas or hemorrhagic complications. The placement of peripheral nerve blocks in sufferers with a coagulopathy should be performed with caution, especially in a deep, noncompressible web site the place an increasing hematoma might go unnoticed. It is imperative that each one preoperative neurologic deficits are documented to enable early analysis of new or worsening neurologic dysfunction postoperatively. Postoperative sensory or motor deficits must even be distinguished from residual (prolonged) native anesthetic impact. Imaging techniques, such as computed tomography and magnetic resonance imaging, are useful in figuring out infectious processes and expanding hematomas. Although most neurologic complications resolve utterly within a number of days or perhaps weeks, vital neural injuries necessitate neurologic consultation to document the degree of involvement and coordinate further workup. Neurophysiologic testing, similar to nerve conduction research, evoked potentials, and electromyography, are often useful in establishing a prognosis and prognosis. Infectious issues could be brought on by exogenous (contaminated treatment or equipment) or endogenous sources. Infection on the site of needle placement is an absolute contraindication to peripheral nerve blockade, although caution ought to be used in sufferers with nearby cellulitis or systemic blood infections (bacteremia or sepsis). Therefore practitioners of regional anesthesia should be familiar with the instant detection and therapy of systemic local anesthetic toxicity. Systemic local anesthetic toxicity can occur instantly from an intravascular injection or it might be delayed because of speedy or extreme systemic absorption of native anesthetic. In addition to frequent aspiration during injection of native anesthetic, the addition of epinephrine can help alert the practitioner to potential intravascular injection. Attaching intravenous tubing to the needle permits immobility of the needle during injection. Typically, an assistant will aspirate with the syringe after every 5 mL injection of native anesthetic. Recent studies indicate that lipid emulsion rescue remedy improves success of resuscitation from cardiac arrest as a outcome of native anesthetic toxicity if given immediately after a neighborhood anesthetic overdose. Many studies have now demonstrated efficacy of ultrasoundguided regional blockade. Ultrasound has the potential to stop and detect two essential antagonistic occasions during peripheral nerve blocks: intravascular injection and intraneural injection of a local anesthetic. Summary and Conclusions Peripheral nerve block strategies benefit the affected person intraoperatively and postoperatively. Successfully mastering these strategies and making use of them to the suitable clinical situations add useful options to the anesthetic care. Knowledge of regional anesthesia can also be essential for the diagnosis and remedy of acute and chronic ache syndromes (see Chapters fifty one and 82). Ultrasound is a guidance tool that many people are electing to choose for regional anesthesia blocks. Once proficiency is established for a selected procedure, beginning to use ultrasound for other interventional functions is comparatively easy. Ultrasound imaging can prevent and detect important occasions corresponding to intravascular or intraneural injection which will improve security during regional anesthesia procedures. However, if safety outcomes are to enhance, then education and coaching play key roles in decreasing these relatively uncommon opposed occasions. Many of these adverse occasions have only been acknowledged in retrospect by the evaluation of recorded sonograms, which is a priceless training apply. One of the unique strategies developed for training novices in ultrasound-guided interventions was use of a tissue-equivalent phantom. In the primary prototype, the phantom and container have been clear; consequently, visual affirmation was attainable. Several phantoms are actually marketed for regional anesthesia purposes, and biologic tissue models that simulate nerve blocks have been developed. Cadavers have the benefit of sensible regional anatomic constructions and can be utilized for simulated interventions. Most training studies have concluded that expertise for ultrasound-guided procedures can be quickly acquired. One training research has identified widespread errors of novices while learning ultrasound-guided regional blocks. Peripheral nerve harm caused by injection needles used in regional anaesthesia: affect of bevel configuration, studied in a rat model. Sonographically guided core-needle biopsy of breast masses: the "bayonet artifact. In-vitro visualization of biopsy needles with ultrasound: a comparative examine of normal and echogenic needles using an ultrasound phantom. Ultrasound visibility of needles used for regional nerve block: an in vitro study. High-resolution ultrasound-guided high interscalene plexus block for carotid endarterectomy. Ultrasound-guided intermediate cervical plexus block and perivascular local anesthetic infiltration for carotid endarterectomy: a randomized controlled trial. Ultrasound-guided deep or intermediate cervical plexus block: the target should be the posterior cervical area.