Generic 25mg persantine otc
Cardiac examination reveals a holosystolic murmur at the lower left sternal border with related gallop and clicks medicine 014 persantine 25mg sale. The area between the true annulus and the displaced valve leaflet is considered "atrialized medicine 3x a day persantine 25 mg buy generic line. Initially, administration of the severely cyanotic infant is aimed toward selling pulmonary blood flow. Supplemental oxygen, inhaled nitric oxide, and mild respiratory alkalosis can have marginal success in enhancing pulmonary blood flow by reducing pulmonary vascular resistance. Options include tricuspid valve restore or substitute, 11/2 ventricle repair, or other palliative procedures such as right ventricular exclusion with a fenestrated patch and placement of a modified Blalock-Taussig shunt (Reemtsen et al, 2007). Although surgical outcomes have improved, a neonatal restore for symptomatic illness stays a danger issue for dying (McElhinney et al, 2005; Sarris et al, 2006). It is theorized that the expansion of developing vascular structures is dependent on circulate. The fetal left ventricle is predominantly crammed with blood that passes via the foramen ovale. Restriction to flow or reversal of circulate by way of the foramen ovale could then end in decreased move to the left heart and its underdevelopment. Similarly, a quantity of studies have documented the progression of severe aortic stenosis to hypoplastic left heart syndrome in utero (Danford and Cronican, 1992; Hornberger et al, 1995). The progressive left ventricular hypertrophy, dilation, and fibrosis associated with extreme aortic stenosis can lead to decreased ventricular compliance, elevated left atrial pressures, and reversal of move via the foramen ovale in utero. Because of the underdevelopment of the left coronary heart buildings, pulmonary venous return must exit the left atrium through the foramen ovale. Pulmonary venous blood then mixes with systemic venous return in the best atrium and enters the proper ventricle. Right ventricular output then passes either to the pulmonary circulation or through the ductus arteriosus to the systemic circulation. The ratio of systemic to pulmonary blood flow is determined by the relative resistances of the vascular beds. As the normal postnatal drop in pulmonary vascular resistance happens, pulmonary flow will increase on the expense of systemic move. Postnatally, prostaglandins are immediately began to keep ductal patency and an echocardiogram is obtained to confirm the diagnosis. The cardiothoracic surgeon and the interventional heart specialist should be made conscious and out there on the time of delivery. In the absence of prenatal analysis, postnatal presentation is considerably variable and depending on ductal patency and the diploma of restriction to flow at the atrial septum. Cyanosis is minimal and pulmonary overcirculation is gentle whereas pulmonary vascular resistance is high. As pulmonary vascular resistance drops and ductal closure occurs, feeding difficulties and respiratory distress become obvious with speedy progression to cardiovascular collapse. Physical exam after ductal restriction is critical for lethargy, pallor, and diminished or absent pulses. Chest radiograph sometimes reveals relatively normal-sized heart and pulmonary edema. Prostaglandins should be started instantly postnatally to ensure ductal patency. Echocardiography is utilized to affirm cardiac anatomy and decide the degree of restriction to flow via the foramen ovale. If the atrial-level shunt is restrictive with profound cyanosis and metabolic acidosis, a balloon atrial septostomy, surgical septectomy, or emergent stage I palliation must be carried out (see later discussion). If the restriction was current in utero, pathologic fibrosis and arterialization of the pulmonary veins and medial hypertrophy of the pulmonary arterioles happens. Even after atrial septostomy, lung disease can persist and pulmonary vascular resistance can remain high. A small group of patients could have adequately balanced pulmonary and systemic blood circulate at the time of presentation. A small diploma of restriction to circulate by way of the foramen ovale could also be related to slight cyanosis however has the beneficial effect of restricting pulmonary blood flow. In the absence of acidosis or end organ dysfunction, this state is generally tolerated until stage I palliation is carried out. An unrestrictive atrial septal defect allows increased pulmonary blood flow as the pulmonary vascular resistance falls. Because of the parallel association of the circulations, growing pulmonary move decreases systemic circulate. The ratio of pulmonary to systemic blood move is balanced by manipulating the resistances of the pulmonary and systemic vascular beds. The success of these therapies is monitored using oxygen saturation, blended venous saturation, lactate, and arterial blood gases. Pulmonary vascular resistance may be manipulated via mechanical air flow and alteration within the amount of oxygen delivered. Only hypercarbia has been proven to enhance systemic oxygen delivery (Tabbutt et al, 2001). The goal of this remedy is to maintain regular lactate, systemic oxygen saturation at 75�85%, and mixed venous oxygen saturation roughly 25 percentage factors lower than systemic saturations. Vasoactive medications can be utilized to alter systemic vascular resistance and enhance ventricular function. Use of these medicines is determined by scientific presentation and echocardiographic findings. Milrinone can be utilized to provide some afterload discount, if tolerated by blood strain. The inotropic effects of milrinone are also a bonus if ventricular perform is poor. In addition to reducing pulmonary blood flow, afterload reduction has the added benefit of lowering tricuspid valve regurgitation whether it is current. Although counterintuitive, when confronted with an unoperated affected person with high oxygen saturations and low peripheral blood strain, the gentle addition of milrinone might improve blood stress just by rising systemic blood circulate. The immediate goal of surgical palliation is to present secure unrestricted systemic and coronary blood circulate and reliably restricted pulmonary blood circulate. The Sano modification has the presumed benefit of providing pulsatile move to the pulmonary arteries without aortopulmonary diastolic run off and coronary metal. A hybrid procedure that mixes stent placement in the ductus arteriosus by the heart specialist and pulmonary artery banding by the surgeon is an method being taken by a quantity of institutions that gives a comparatively noninvasive stage I palliation for hypoplastic left heart syndrome (Caldarone et al, 2007). Each of those procedures has its execs and cons and its advocates and detractors (Caldarone et al, 2007; Ghanayem et al, 2006; Malec et al, 2003). Longer-term prospective studies are wanted to decide the optimal strategy to stage I palliation. The superior cavopulmonary anastomosis (bidirectional Glenn) is normally carried out between four and 6 months of age. During this process, the conduit providing pulmonary flow is removed and the superior vena cava is anastomosed to the pulmonary artery.
25 mg persantine purchase visa
Hindricks G treatment 0 rapid linear progression 100mg persantine buy with mastercard, Willems S symptoms jaw pain and headache discount 25mg persantine with amex, Kautzner J, et al: Effect of electroanatomically guided versus conventional catheter ablation of typical atrial flutter on the fluoroscopy time and useful resource use: a potential randomized multicenter examine. Bru P, Duplantier C, Bourrat M, et al: Resumption of right atrial isthmus conduction following atrial flutter radiofrequency ablation. Vijayaraman P, Dandamudi G, Naperkowski A, et al: Adenosine facilitates dormant conduction across cavotricuspid isthmus following catheter ablation. Chen J, de Chillou C, Basiouny T, et al: Cavotricuspid isthmus mapping to assess bidirectional block throughout widespread atrial flutter radiofrequency ablation. Poty H, Saoudi N, Nair M, et al: Radiofrequency catheter ablation of atrial flutter. Further insights into the assorted kinds of isthmus block: software to ablation during sinus rhythm. Tada H, Oral H, Sticherling C, et al: Double potentials alongside the ablation line as a information to radiofrequency ablation of typical atrial flutter. Oral H, Sticherling C, Tada H, et al: Role of transisthmus conduction intervals in predicting bidirectional block after ablation of typical atrial flutter. Navarrete A, Conte F, Moran M, et al: Ablation of atrial fibrillation at the time of cavotricuspid isthmus ablation in sufferers with atrial flutter with out documented atrial fibrillation derives a greater long-term benefit. Nakagawa H, Shah N, Matsudaira K, et al: Characterization of reentrant circuit in macroreentrant proper atrial tachycardia after surgical restore of congenital heart disease: isolated channels between scars enable "focal" ablation. Ouyang F, Ernst S, Vogtmann T, et al: Characterization of reentrant circuits in left atrial macroreentrant tachycardia: important isthmus block can stop atrial tachycardia recurrence. Reports as early as 190710 implicated a number of quickly firing foci as a mechanism. In this chapter, epidemiology, nomenclature, present mechanistic insights, and up to date therapy strategies might be mentioned. These wavelets are continuously topic to extinction or era of latest circuits (daughter wavelets). Genetic predisposition, stretch, neurohormonal milieu, and modifications in autonomic tone have all been implicated. Secular developments in incidence of atrial fibrillation in Olmsted county, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Selection of antithrombotic brokers consists of antiplatelet therapy (aspirin with or without clopidogrel), vitamin K antagonists (warfarin), and newer anticoagulants such because the direct thrombin inhibitor dabigatran and direct factor Xa inhibitors rivaroxaban and apixaban. Although the bleeding risk is higher, warfarin is superior to aspirin in reducing thromboembolic events. Dabigatran was reported to have a similar or lower stroke and major bleeding risk and a decrease in hemorrhagic strokes in contrast with warfarin, without a difference in overall mortality. Other options for stroke prevention, notably in sufferers with contraindications to anticoagulation, are surgical or percutaneous left atrial appendage exclusion or occlusion. Reductions in the long term danger for stroke after surgical exclusion of the left atrial appendage, even among patients with excessive baseline danger components and tons of who discontinued anticoagulation following surgery, have been reported. Early studies instructed a major effect of operator experience and a studying curve in minimizing the danger of issues. Large-scale randomized trials might be necessary to determine whether there shall be a reduction in the risk of stroke. The lenient technique was noninferior to a strict fee management strategy within the composite main end result (death from cardiovascular causes, hospitalization for heart failure, stroke, systemic embolism, bleeding, and life-threatening arrhythmias). Some patients with left ventricular dysfunction and heart failure could benefit with preliminary biventricular pacing on the time of ablation, but this subset remains to be better defined. In sufferers who experience a lower in cardiac perform following right ventricular pacing, an improve to a biventricular pacing device can provide subsequent enchancment in ejection fraction and heart failure symptoms. Circulation 114:759�765, 2006; Guiot A, Jongnarangsin K, Chugh A, et al: Anticoagulant therapy and threat of cerebrovascular events after catheter ablation of atrial fibrillation in the elderly. However, its potential cumulative systemic side effects are a concern and must be monitored rigorously. Lacking the iodine moiety, dronedarone was proposed to have fewer opposed results than amiodarone; nonetheless, it appears to be much less effective. Simvastatin attenuates atrial tachycardia pacing�induced electrophysiological reworking via inhibition of the downregulation of L-type calcium channels, and it reduces atrial fibrosis and conduction abnormalities by attenuating fibroblast proliferation. A recent metaanalysis of nine studies together with 6400 sufferers demonstrated that uninterrupted anticoagulation with warfarin throughout ablation significantly decreased the thromboembolic risk with out an elevated risk of bleeding. Therapeutic anticoagulation is routinely continued for three months or longer after ablation. The decision to discontinue anticoagulation after ablation is based on inherent thromboembolic danger, particularly age and history of prior stroke, efficacy of ablation in eliminating atrial arrhythmias, and patient and doctor choice. In patients in whom anticoagulation with warfarin or newer anticoagulants is discontinued, use of aspirin ought to be thought of indefinitely. The left atrial roof, mitral isthmus, posterior mitral annulus, inferoposterior wall of the left atrium, septal side of the left atrium, and anterior wall are frequently focused websites. Because conduction gaps along the traces can facilitate macroreentrant atrial flutters, it is essential to obtain full conduction block each time linear ablation is tried. Identification of acceptable targets for ablation based mostly on electrogram analysis is a quickly evolving approach that relies on the power to process and analyze indicators on an actual time foundation. This promising strategy would require detailed examination of the mapping algorithms and validation in multicenter randomized studies. Adjunctive methods could be tailor-made to the individual patient and depend upon operator choice. Thesamepercentiles are additionally shown for the cumulative burden of atrialfibrillation. Based on an 80% efficacy fee for sinus rhythm maintenance, relative reduction in stroke threat would want to be greater than or equal to 42% or 11% to understand price effectiveness ratios of lower than $50,000 and $100,000, respectively, per quality adjusted life yr. Uninterrupted warfarin all through the perioperative interval has proven a reduction in periprocedural stroke with out a rise in bleeding danger. Technological advances in mapping and ablation methods have established catheter ablation as a protected and effective option for many sufferers. Development of novel atrioselective antiarrhythmic pharmacologic agents which might be secure and efficient should also be helpful. Sahadevan J, Ryu K, Peltz L, et al: Epicardial mapping of continual atrial fibrillation in patients: Preliminary observations. Oral H, Ozaydin M, Chugh A, et al: Role of the coronary sinus in upkeep of atrial fibrillation. Haissaguerre M, Hocini M, Takahashi Y, et al: Impact of catheter ablation of the coronary sinus on paroxysmal or persistent atrial fibrillation. Atienza F, Almendral J, Jalife J, et al: Real-time dominant frequency mapping and ablation of dominant frequency websites in atrial fibrillation with left-to-right frequency gradients predicts longterm upkeep of sinus rhythm. Yoshida K, Chugh A, Good E, et al: A important decrease in dominant frequency and scientific consequence after catheter ablation of persistent atrial fibrillation. Katritsis D, Giazitzoglou E, Sougiannis D, et al: Complex fractionated atrial electrograms at anatomic sites of ganglionated plexi in atrial fibrillation. Structural, practical, and electrophysiological characteristics of a new model of sustained atrial fibrillation. Sohara H, Amitani S, Kurose M, et al: Atrial fibrillation activates platelets and coagulation in a time-dependent manner: A research in patients with paroxysmal atrial fibrillation.
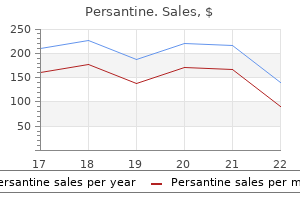
| Comparative prices of Persantine |
| # | Retailer | Average price |
| 1 | Aldi | 479 |
| 2 | BJ'S Wholesale Club | 328 |
| 3 | Menard | 341 |
| 4 | Brinker International | 354 |
| 5 | ShopRite | 357 |
| 6 | Save Mart | 256 |
| 7 | Publix | 210 |
| 8 | Safeway | 950 |
| 9 | PetSmart | 368 |
| 10 | Williams-Sonoma | 147 |
Cheap persantine 25mg
Klein et al (2007) just lately found the gene responsible for classical autosomal recessive extreme congenital neutropenia treatment keratosis pilaris persantine 25 mg discount line, first described by Kostmann (1956) medicine assistance programs cheap 100mg persantine otc. The mechanism for a way these mutations are acquired and the way they predispose to leukemia remains to be under investigation. This deficiency ends in accumulation of glycogen in the liver, kidneys, and intestines. Presenting features could encompass any of the following: acute metabolic derangement, failure to thrive, recurrent infections, muscular hypotonia, and delayed psychomotor growth (Rake et al, 2002). Lack of transport of glucose 6-phosphate could impair mobile perform and result in apoptosis (Hiraiwa et al, 1999; Kilpatrick et al, 1990). Immunologic and hematologic investigations in patients with recurrent infections revealed the presence of continual noncyclic neutropenia and lymphopenia. Neutropenia may be due to an arrest of myeloid maturation, with underproduction of mature neutrophils and diminished bone marrow storage swimming pools. Lymphopenia, decreased delayed hypersensitivity, and impaired in vitro responsiveness of lymphocytes to mitogens recommend useful dysfunction of small lymphocytes (Lux et al, 1970). Neutrophils and macrophages play important roles as effector cells in the phagocytic system. The efficient perform of the phagocyte system is determined by a quantity of components, including the presence of sufficient numbers of phagocytes in the peripheral blood, the power to reply to alerts from the sites of inflammation, the ability to migrate to these sites, and the aptitude to ingest and kill invading microorganisms. These receptors are important in initiating and orchestrating the immune response. Clinical manifestations begin in neonates with diarrhea, weight reduction, failure to thrive, eczema, otitis media, and pneumonia. By 2 years of age, dwarfism is clear; later, gait disturbances end result from metaphyseal chondrodysplasia. Aplastic anemia occurs in about 25% of the instances, and leukemic transformation has been described. Allogeneic bone marrow transplantation is the only treatment for this bone marrow failure syndrome. Reticular Dysgenesis Reticular dysgenesis is characterized by extremely extreme neutropenia, leukopenia, agammaglobulinemia, and presence of rudimentary thymic, lymphoid, and splenic tissue. In the bone marrow, erythroid and megakaryocyte elements are regular, but myeloid cells are absent or sparse, presumably owing to a maturation defect in a progenitor cell (Roper et al, 1985). Allogeneic bone marrow transplantation stays the one out there curative option. Barth Syndrome Barth syndrome is an X-linked recessive disorder characterised by neutropenia, cardiomyopathy, skeletal myopathy, progress deficiency, and 3-methylglutaconic aciduria. A current examine demonstrated neutropenia in 25% of sufferers, however normal hematocrit and platelets (Spencer et al, 2006). Myelokathexis is recognized by hypersegmented neutrophils with increased apoptosis (Zuelzer, 1964). The innate immune response features as the primary line of defense towards infection. It consists of soluble factors, corresponding to complement proteins, and diverse mobile components, together with granulocytes (basophils, eosinophils, and neutrophils), mast cells, macrophages, dendritic cells, and pure killer cells. The adaptive immune response is slower to develop but manifests as increased antigenic specificity and memory. Natural killer T cells and T cells are cytotoxic lymphocytes that straddle the interface of innate and adaptive immunity. The immaturity of neonatal host defense is also characterised by profound deficiencies in quantitative and qualitative phagocytic effector cell perform. Stressed and septic neonates exhibit vital dysfunction of the phagocytic course of. Chemotaxis is a process that entails quite a few modifications in mobile motility and mobility, adopted by intracellular biochemical changes. It begins with stimuli from the invading microorganism and continues with the directed migration of neutrophils to the location of invasion, ingestion of the pathogen, and killing by oxygen-dependent and -independent mechanisms. Qualitative abnormalities of neonatal neutrophils embrace decreased deformability and impaired features including chemotaxis, phagocytosis, adherence, bacterial killing, aggregation, and oxidative metabolism (Cairo et al, 1990b). Significant defects in the upregulation of surface-active glycoprotein receptors (C3bi) and lowered aggregation also predispose the neonate to impaired response to bacterial an infection. These unfavorable growth elements regulate early hematopoiesis with suppressive results on the proliferation of early myeloid and lymphoid progenitors. Monocytes are present in high proportions within the early hematopoietic tissues, with roughly 70% of hematopoietic cells at four. This proportion decreases to 1% to 2% over the following 6 weeks as erythroid cells turn out to be predominant. The estimated complete bone marrow cellularity of the term neonate at delivery is roughly 1. These levels remain low by way of the neonatal interval, by which circulating monocyte counts are highest in the 1st week of life, starting from 1340 to 2200 cells/L, and gradually fall in successive weeks to seven-hundred cells/mm3 at three weeks and 450 cells/mm3 by 6 years of age. Morphology Immunophenotyping using fluorescent conjugated monoclonal antibodies additionally has been used to determine monocyte cell subpopulations and give perception to cell activation and performance. FcR receptors are necessary in the means of monocyte and macrophage phagocytosis of microbes and antibodydependent cytotoxicity. Monocytes are capable of directed movement (chemotaxis) in response to substances (chemokines) produced by micro organism or by accessory cells on the website of injury or invasion. Chemotactic capabilities of neonatal and adult peripheral blood monocytes have been compared, and chemotaxis was discovered to be less pronounced in neonates than in adults (Table 78-3). Finally, the activated monocyte moves via the endothelium to the site of irritation or an infection. Preliminary studies show that ranges of monocyte adhesion molecule expression are comparable in neonate and grownup peripheral blood (Schibler, 2000). The capacity of monocytes of fetal and neonatal monocytes to kill pathogens (Staphylococcus aureus, S. They have the ability to lyse target cells and secrete immunomodulatory cytokines (Robertson and Ritz, 1990). The bone marrow then stays the first website of maturation (Miller et al, 1992; Shibuya et al, 1993). After activation, lysosome-like vesicles containing perforin, serine esterases, and sulfated proteoglycans are secreted toward the target cell. Proteoglycans defend the granzymes from inactivation by protease inhibitors (Berthou et al, 1995; Moretta et al, 2005; Pao et al, 2005; Robertson and Ritz, 1990; Spaeny-Dekking et al, 2000). These cytokines help to recruit macrophages and different antigen-presenting cells for more efficient control of the infection (Cooper et al, 2001a, 2001b). Laboratory evaluation reveals cytopenias, liver dysfunction, hypofibrinogenemia, hypertriglyceridemia, hypoalbuminemia, and hyponatremia. Treatment might embrace chemotherapy and/or hematopoietic stem cell transplant (Filipovich, 2008). Unlike different severe inherited neutropenias, there are mature neutrophils present in the bone marrow.
Purchase 25 mg persantine with mastercard
Recoarctation happens in 10% to 15% of kids and is efficiently managed with balloon angioplasty treatment of lyme disease buy cheap persantine 25mg line. If a ventricular septal defect is present medicine 2 times a day order persantine 25 mg with amex, this is typically closed on the time of surgery. Dashed lines point out the potential areas of discontinuity (interruption) in the aortic arch. Aberrant preparations of the head and neck vessels are widespread, with 50% of patients with kind B interruption having an aberrant proper subclavian artery that arises from the descending aorta. The scientific presentation of interrupted aortic arch is similar to that of different left-sided obstructive lesions. Surgical restore is carried out after metabolic acidosis resolves and end-organ function is improved. In sufferers with extreme left ventricular hypoplasia, a two-ventricle repair may not be potential and a staged restore or single-ventricle palliation is carried out (Tchervenkov et al, 2005). Surgical mortality is lower than 10%, but higher in sufferers with extra anomalies (Brown et al, 2006). Repeat operation as a end result of left ventricular outflow tract obstruction and balloon angioplasty for recurrent arch obstruction are both widespread. As pulmonary artery pressures drops postnatally, perfusion pressure of the left coronary artery falls, resulting in ischemia and infarction of the left ventricle. If collateral vessels join the right and left coronary circulations, circulate in the left coronary artery reverses. Mitral valve regurgitation secondary to papillary muscle ischemia and left ventricular dilation develops. If enough collateral vessels and myocardial oxygen supply exist, the patient may present later in life with angina-like symptoms. In the infant, assaults of irritability, pallor, and diaphoresis with feeds are a typical presentation. Cardiac examination reveals a displaced level of most impulse, gallop rhythm, and nonspecific murmur. If mitral regurgitation is current, a holosystolic, regurgitant-quality murmur is heard. Color Doppler could show retrograde circulate in the left coronary with flow into the pulmonary artery. Surgical reimplantation of the left coronary artery to the aorta restores regular coronary perfusion stress. If myocardial injury is severe or the left coronary artery is unable to be reimplanted surgically, cardiac transplantation is performed. Hemangiomas are tumors that demonstrate endothelial hyperplasia and endure a period of proliferation and involution. They have regular endothelial cell turnover and grow accordingly with surrounding constructions. Vascular malformations are further subcategorized by the type of vascular tissue concerned (arterial, venous, and lymphatic). An effective massive left-to-right shunt happens through the direct arterial-venous connections. A, the department pulmonary arteries and arch vessels are snared, and a ligature is positioned across the ductus arteriosus. To adequately mobilize the descending aorta, the left subclavian artery could need to be divided (as shown). After resection of the ductus arteriosus, the proximal (pulmonary artery) end is oversewn. An various technique is anastomosis of the left subclavian and left frequent carotid arteries mixed with homograft patch augmentation of the inferior floor of the arch. The increased systemic venous return will increase right atrial pressures and promotes right-to-left shunting by way of the foramen ovale. Systolic murmurs could also be current secondary to tricuspid valve regurgitation or increased move across the pulmonary valve. When a malformation is suspected, care should be taken to auscultate areas the place malformations are probably, corresponding to the pinnacle, liver, and chest. Arteries proximal to the malformation are sometimes dilated with bounding pulses, whereas those distal are small with diminished pulses. Treatment, if necessary, requires interventional closure or surgical ligation of the anomalous vascular connections. There is a paucity of data, nonetheless, concerning the prognosis and administration of fetal and new child cardiomyopathy. In evaluating a newborn infant with indicators of congestive coronary heart failure, structural coronary heart illness must be dominated out. In the absence of structural problems, the prognosis of cardiomyopathy should be considered. The etiology of neonatal cardiomyopathy contains prenatal infections (with cytomegalovirus, human immunodeficiency virus, enterovirus, or parvovirus); familial or genetic causes; maternal autoimmune disease with anti-Ro or anti-La antibodies; prenatal drug publicity; arrhythmia-induced cardiomyopathy; and twin-twin transfusion. Initial stabilization may require mechanical ventilation, the utilization of ionotropes, afterload discount, and diuresis. Long-term treatment is dependent somewhat on the specific cause of the cardiomyopathy, because some varieties may be reversible. Since then, improved understanding of transplant immunology and medical management has made heart transplantation in infants and kids an essential choice in inoperable patients or these with end-stage cardiac disease. In a current scientific assertion from the American Heart Association, the indications for pediatric heart transplantation have been outlined (adapted from Canter et al, 2007): 1. Progressive deterioration of ventricular perform or useful status despite optimum medical care four. Malignant arrhythmia or survival after cardiac arrest unresponsive to medical therapy, catheter ablation, or an computerized implantable defibrillator 5. Growth failure secondary to severe congestive coronary heart failure unresponsive to conventional medical remedy 7. Unacceptably poor high quality of life There are quite so much of lesions within the neonate for which cardiac transplantation has been used as major palliation. For example, over the previous decade, survival of patients present process surgical palliation of hypoplastic left coronary heart syndrome has continued to enhance (Alsoufi et al, 2007; Gordon et al, 2008). With the availability of infant donors growing only barely over this interval of time (Table 55-2), the steadiness for treatment of those newborns has shifted toward surgical palliation with the Norwood or hybrid Norwood procedures. Patients with the other lesions simply noted proceed to have comparatively poor surgical outcomes, suggesting that palliation with heart transplantation may be one of the best method. The long-term survival of infants who endure heart transplantation is quite good. The calculated "half-life" of transplant recipients younger than 1 12 months of age was 15.
Persantine 100mg sale
Current proof strongly suggests that intravenous lipids may be administered to sick preterm infants in early postnatal life with out inflicting acute metabolic derangements symptoms xeroderma pigmentosum persantine 100mg cheap mastercard. Concern concerning the long-term safety of early intravenous administration of lipids symptoms ptsd generic persantine 100 mg visa, significantly the potential of an increase in mortality and bronchopulmonary dysplasia, was raised by some early observational studies. In view of those knowledge and of the essential fatty acid and caloric needs of sick untimely infants, early intravenous lipid administration (on day 1 of life) is a beneficial clinical practice. The fee of intravenous lipid infusion is essential, and plasma lipid clearance is improved when intravenous lipid is given as a steady infusion over 24 hours (Putet, 2000). Lipid infusion rates well beneath this worth can easily be achieved in clinical follow if lipids are offered over 24 hours in an amount not exceeding three to four g/kg/day. This level of lipid consumption is normally sufficient to provide the caloric needs of preterm infants (in combination with glucose) and is normally tolerated by premature infants. Triglyceride concentrations are most frequently used as a sign of lipid tolerance, and maintaining triglyceride concentrations below 150 to 200 mg/dL seems desirable. Numerous studies have documented superiority of 20% over 10% lipid emulsions (Putet, 2000). Lipid clearance is improved with the 20% solutions as a end result of these options have half the amount of phospholipid emulsifier relative to the identical quantity of triglycerides. Phospholipids can mix with cholesterol to kind lipoprotein X, which finally interferes with the clearance of infused triglycerides. Concern has been expressed about the use of intravenous lipids in infants with hyperbilirubinemia, as a result of free fatty acids may displace bilirubin from albuminbinding sites, potentially increasing the chance of kernicterus. Although the clinical significance of this finding is unsure, it may be cheap to think about lowering intravenous lipids in extremely premature infants with vital hyperbilirubinemia. Intravenous lipid emulsions might undergo lipid peroxidation, with the formation of natural free radicals, probably initiating tissue harm. Light, especially phototherapy, could play some position in increasing lipid peroxidation in intravenous lipid emulsions (Neuzil et al, 1995). However, multivitamin preparations included within the intravenous solutions are main contributors to era of peroxides, and lipid emulsions could have only a minor additive impact (Lavoie et al, 1997). On the basis of these findings, some clinicians defend intravenous lipid solutions from gentle, though the significance or clinical efficacy of this practice stays unsure. Only a large randomized clinical trial is prone to resolve this concern (Sherlock and Chessex, 2009). Carnitine facilitates transport of long-chain fatty acids by way of the myocardial membrane and thereby plays an necessary function of their oxidation. Premature infants receiving parenteral diet have low carnitine levels, but the scientific significance of this discovering remains unsure. Metaanalysis of the studies evaluating carnitine supplementation in parenteral diet confirmed no evidence of effect on ketogenesis, lipid utilization, or weight achieve (Cairns and Stalker, 2000). At present, insufficient data is out there to support a recommendation for the routine supplementation of parenterally fed neonates with carnitine. It is, nonetheless, essential to incessantly measure sodium concentrations and water steadiness. Chloride requirements follow the identical time course as for sodium requirements and likewise are 2 to four mEq/kg/day. Potassium intakes of two to 3 mEq/kg/day are often sufficient to maintain normal serum potassium concentrations. Parenteral nutrition options normally require the addition of anions, as both acetate or chloride. In basic, extra anions must be supplied as acetate so as to forestall hyperchloremic metabolic acidosis. A randomized controlled trial demonstrated that acetate in parenteral nutrition solutions successfully ameliorates acidosis (Phelps and Cochran, 1989). Supplying calcium and phosphorus in parenteral nutrition stays a major clinical problem because of restricted solubility. It is presently not possible to provide sufficient calcium and phosphorus to help enough bone mineralization in preterm infants utilizing the options obtainable within the United States. Precipitation of calcium and phosphorus stays a problem in the United States, nonetheless, and the solubility of calcium and phosphorus in parenteral diet options depends on temperature, kind and concentration of amino acid, glucose focus, pH, sort of calcium salt, sequence of addition of calcium and phosphorus to the solution, the calcium-to-phosphorus ratio, and the presence of lipid. Adding cysteine to parenteral diet solutions lowers the pH, which improves calcium and phosphorus solubility. In general, calcium and phosphorus must be added to parenteral diet options in early postnatal life. Calcium, phosphorus, and magnesium serum concentrations ought to be incessantly monitored. There is cheap consensus that zinc should be included early in parenteral diet options (250 g/kg/day for time period infants, four hundred g/kg/day for preterm infants). The really helpful intakes of hint components for term and preterm infants are proven in Table 67-4. Several pediatric trace steel solutions can be found that contain zinc, copper, magnesium, and chromium in various proportions; these options are usually offered at zero. When hint metallic solutions are used, extra zinc normally is needed to provide the beneficial intake for preterm infants. Supplementation with selenium is usually recommended after 2 weeks of age, as a end result of preterm infants can turn out to be selenium deficient after 2 weeks of unique parenteral diet. In infants with cholestasis, copper and manganese must be discontinued, and chromium and selenium should be used with warning and in smaller quantities in infants with renal dysfunction. At present, parenteral iron is really helpful solely when preterm infants are nourished exclusively by parenteral solutions for the first 2 months of life. The really helpful intakes of vitamins for term and preterm infants on parenteral diet are shown in Table 67-5. These dosages present greater quantities of many of the B nutritional vitamins and decrease quantities of vitamin A relative to the recommendations. Recommendation is made with warning due to very limited expertise with intravenous iron in infants and lack of a secure, acceptable intravenous preparation (estimated daily intravenous requirement is one hundred g/kg for term infants and 200 g/kg for preterm infants). Many of the complications (electrolyte and glucose imbalance) may be prevented or corrected by manipulating the constituents of the infusate. The primary issues of parenteral diet as currently used are cholestasis and those associated to the infusion catheter. Cholestatic jaundice because of hepatic dysfunction is a well-recognized complication of parenteral vitamin. The preliminary histologic lesion is cholestasis, both intracellular and intracanalicular, followed by portal inflammation and progression to bile duct proliferation after a quantity of weeks of parenteral diet. Cholestasis most often resolves after discontinuation of parenteral vitamin and initiation of enteral feedings. Some uncommon situations of irreversible liver failure have been documented, however this seems to happen solely after a number of months of use. The most regularly recognized risk components in parenteral nutrition�associated cholestasis are length of parenteral diet, diploma of immaturity, and delayed enteral feeding (Steinbach et al, 2008). There is expanding proof that even small-volume enteral feedings can cut back the incidence of cholestasis. Early research of parenteral diet suggested a attainable relationship between the amount of amino acids and hepatic dysfunction.
Syndromes
- Turn the television off during mealtimes, homework time, and other times of day during which social interaction and learning are going on.
- Problems swallowing
- Chorionic villous sampling
- Follow you closely to make sure the program works for you
- Get a lot of rest. Have someone else do household chores.
- Congenital heart disease (heart problems that are present at birth)
- Fever
25 mg persantine generic overnight delivery
Catecholamine Secretion A hallmark of neuroblastoma cells is the ability to retailer and secrete catecholamines symptoms quitting weed trusted 100mg persantine. Patients with neuroblastoma usually have elevated urinary levels of norepinephrine as nicely as its biochemical precursors and their metabolites gas treatment purchase 25 mg persantine free shipping. In the occasional case with no elevation of catecholamines, a 24-hour urine collection is important. Urine catecholamines should be measured earlier than surgical removing of the tumor or before initiation of therapy. Catecholamine secretion can be utilized not only as a diagnostic assist but also as a means to assess the response to therapy and to detect tumor recurrence. Bilateral bone marrow aspiration (along with bilateral bone marrow biopsy in sufferers over age 6 months) is also part of the preliminary analysis. Because tumor-specific biologic data performs a crucial role in danger classification and therapy recommendations, acquiring sufficient tissue for biologic research is essential. The most widely used morphologic classification system is predicated on that proposed by Shimada, by which tumors are categorized as favorable or unfavorable (Sano et al, 2006; Shimada et al, 1999). Classification depends on age, the degree of differentiation of the neuroblasts, the cellular turnover (mitosis-karyorrhexis) index, and the presence or absence of Schwannian stromal development. Common genomic aberrations present in neuroblastoma embrace deletion on the chromosomal region 1p36. Comprehensive genome-wide approaches corresponding to comparative genomic hybridization have gotten more and more useful in refining the prognostic accuracy of chromosomal alterations (Schleiermacher et al, 2007). Genetic Prognostic Factors: Tumor Biology In addition to scientific elements and histology, a selection of biologic elements have been shown to correlate with prognosis (Table 80-6). Infants with hyperdiploid tumors have a significantly better response to therapy than these with diploid tumors (Bourhis, 1991). Infants with stage 4S illness have a very good prognosis regardless of having disseminated illness; spontaneous regression happens with out cytotoxic remedy in approximately 50% of cases. Treatment Treatment modalities for neuroblastoma include observation alone, surgery, chemotherapy, and radiation therapy. Factors that have an effect on end result embody the age at diagnosis, stage of illness, histology, and tumor biology (see Table 80-6). Patients with stage 1 and stage 2 neuroblastoma have a 96% to 100 percent survival price with surgical procedure alone (Perez et al, 2000). Infants with stage three and stage 4 illness have a poorer survival, even with aggressive chemotherapy, although the end result, with better than 70% surviving overall, is a lot better than the 10% to 20% reported for older kids with these levels (Schmidt et al, 2000). Infants with stage 4S illness have a very good prognosis, with a 5-year survival >90%, despite having disseminated disease. The unpredictable course of neuroblastoma, with its occasional spontaneous maturation or regression, not only makes this tumor unusual but in addition causes problem in planning remedy. An exception to this rule is in the case of spinal wire compression, by which immediate decompression with chemotherapy, laminectomy, or native irradiation may be used to preserve operate. There is an growing pattern to use chemotherapy first, given the beautiful sensitivity of the tumor to chemotherapeutic brokers, but a fast deterioration in neurologic function should prompt alternative interventions. The combination of intensive laminectomy with postoperative irradiation should be prevented as a outcome of later spinal deformity is nearly inevitable. Infants with stage 3 and stage 4 disease often are handled with combination chemotherapy and local surgery, with radiation therapy given solely as necessary to eradicate residual disease. Active drugs which are mostly used embody cisplatin, etoposide, doxorubicin, cyclophosphamide, vincristine, and ifosfamide. In these high-risk patients, intensive chemotherapy adopted by myeloablative remedy and stem cell assist might provide additional profit (Canete et al, 2009). In addition, using the differentiation agent cis-retinoic acid has been shown to improve survival in sufferers with advanced-stage, high-risk neuroblastoma (Matthay et al, 2009). Infants with stage 4S disease have a highly favorable prognosis and may require minimal or no remedy. Because many patients bear spontaneous regression without chemotherapy and the overall disease-free survival fee is 85% to 90%, therapy must be directed toward supportive care, with use of chemotherapy and surgical procedure restricted to relieving symptoms (De Bernardi et al, 2009). The major cause of demise in these patients is very large hepatic involvement leading to respiratory insufficiency or compromise of renal or gastrointestinal function. Prenatal Diagnosis Neuroblastoma is more and more being detected prenatally by screening ultrasonography. Newborns with adrenal or different mass lesions detected prenatally should be evaluated with urine catecholamines and follow-up ultrasonography. Careful observation could also be sufficient for infants with localized tumors, which frequently regress. Newborn Screening Newborn screening for neuroblastoma by measuring urine catecholamines has been studied in Japan and a variety of different international locations (Hiyama et al, 2008). It was hoped that early diagnosis of neuroblastoma would scale back the frequency of cases with poor prognosis from advanced-stage illness. Screening, however, has shown no influence on survival; neuroblastomas detected by screening nearly all the time have favorable biologic options (Schilling et al, 2002). Two thirds of congenital leukemia circumstances come up from the myeloid lineage, in distinction to older infants and kids in whom acute lymphoblastic leukemia predominates. Congenital leukemia is related to a high mortality with an general survival at 24 months of solely 23% (Bresters et al, 2002); this is as a outcome of of the aggressive biology of these leukemias and to treatment problems. In infants and older kids, numerous elements are associated with the development of leukemia; these embody genetic components, environmental influences, viral infections, and immunodeficiency. Leukemia-associated gene rearrangements have been retrospectively recognized in archived newborn blood spots of children who subsequently developed leukemia (Hjalgrim et al, 2002; Taub et al, 2002; Wiemels et al, 2002). Intrauterine publicity to topoisomerase 2 inhibitors could additionally be responsible for some instances of infant leukemia (Pui and Evans, 1999; Ross, 2000). Nucleotides concerned in the breakpoint of the 11q23 locus could also be particularly prone to topoisomerase 2�induced breaks (Strick et al, 2000). Clinical Manifestations Clinical indicators of leukemia could additionally be evident at start and embody hepatosplenomegaly, petechiae, and ecchymoses. Patients typically have a number of nodules which would possibly be freely movable over the subcutaneous tissue (Resnik and Brod, 1993). There is usually a greenish-blue discoloration of the overlying pores and skin due to the abundance of myeloperoxidase-hence the name chloroma. It is important to carry out cytogenetic studies, in addition to move cytometry, on the pores and skin biopsy specimen; infants found to have an 11q23 rearrangement have a poor prognosis even in the absence of marrow involvement and ought to be handled aggressively (Zhang et al, 2006). When chloromas are current on the top or neck, imaging research ought to be obtained to assess for the presence of intracranial or skull involvement. At delivery, many infants have respiratory misery from leukemic infiltration in the lungs. Severe respiratory issue may develop soon after delivery from pulmonary hemorrhage secondary to thrombocytopenia.
Persantine 25 mg discount with mastercard
However medicine wheel persantine 25 mg buy generic on line, if the toddler reveals no neurologic signs within the perinatal interval medicine 801 cheap 100 mg persantine with mastercard, the outcome is usually regular. Cerebral edema resulting from hypoxia-ischemia is maximal between 36 and 96 hours and may impair cerebral blood flow secondary to elevated intracranial pressure. Attempts to decrease intracranial stress by managed hyperventilation (Paco2 of 20 to 25 mm Hg) in addition to by way of furosemide or mannitol may actually be dangerous (Collins et al, 2001). In one other predictive mannequin, the next elements had been included: the need for chest compressions for >1 minute, delayed onset of respirations >30 minutes, and base deficit >16 throughout the 1st hour of life, had been predictive of poor outcome. The period of the neurologic abnormalities is usually helpful in predicting long-term neurologic disability. In two separate research, normal examination findings at 1 week and at 2 weeks of age correlated with an excellent outcome (Robertson and Finer, 1985; Sarnat and Sarnat, 1976). Hypothermia therapy may confound the predictability of degree of encephalopathy at the completion of remedy. In a secondary evaluation of the Cool-Cap hypothermia trial, the outcomes for newborns after remedy was not essentially reflected in enchancment within the grade of encephalopathy, which may be as a end result of different elements such as using morphine or other sedating medication throughout cooling (Gunn et al, 2008). As with different medical measures, neither of those tools is in a position to prognosticate consequence in the moderately asphyxiated newborn. Study outcomes have various in accordance with the timing of the scan in relation to the damage. It has been reported that the lactate level of the injured brain increases within the first 24 hours and remains elevated thereafter, presumably due to vitality failure and the need to metabolize glucose anaerobically (Hanrahan et al, 1996; Penrice et al, 1996). Outcome the outcome for hypoxic-ischemic mind damage differs substantially for the preterm infant and the time period toddler. Although extra preterm infants survive such an insult than term infants, preterm survivors usually have a tendency to have neurodevelopmental disabilities. In a recent research of extraordinarily preterm youngsters, 49% had disabilities, with 23% assembly standards for extreme disabilities (Wood et al, 2000). In time period infants with neonatal encephalopathy, the presence of seizures and the severity and duration of encephalopathic state are predictors of poor end result (Glass et al, 2009; Robertson et al, 1989; Thornberg et al, 1995). The neurologic examination at 3 months may be an excellent prognostic indicator (Hajnal et al, 1999). In one cohort examine, these with predominant harm to the deep gray nuclei experienced more severe outcomes at 30 months in comparison with these with predominant watershed region injury (Miller et al, 2005b). In particular, absence of the signal within the posterior limb of the internal capsule has been related to poor neurodevelopmental consequence. The term neonatal stroke is reserved for occasions occurring between start and the tip of the first month of life (Raju et al, 2007). Perinatal stroke is more and more acknowledged in full-term infants with an incidence of 1 per 2300 to 4000 liveborn infants (Kirton and deVeber, 2009; Nelson and Lynch, 2004; Schneider et al, 2004; Schulzke et al, 2005). Other symptoms embrace encephalopathy, abnormalities of tone, feeding issues, or apnea. These infants current later with pathologic early hand choice and/or seizures (Golomb et al, 2001). The National Hospital Discharge Survey, from 1980 through 1998, decided that for infants youthful than 30 days of age, the in-hospital mortality price for neonatal stroke was 10. A related evaluate concluded that greater than 50% of youngsters with neonatal stroke seem regular by 12 to 18 months of age (de Vries et al, 1997). Despite these impairments, most kids stroll independently by 2 years of age (Golomb, 2009). The presence of prothrombotic disorders, especially presence of issue V Leiden deficiency, was associated with poor end result in time period infants (Mercuri, 2001). Presence of venous infarction and refractory seizures has been associated with neurologic sequelae (Carvalho et al, 2001; deVeber and Andrew, 2001; Shevell et al, 1989). Increased signal intensity is seen in the proper parietal and frontal areas and the left posterior parietal region. It is being increasingly diagnosed in latest years, most likely reflecting using more delicate neuroimaging methods. Risk elements are much like these for ischemic stroke, with thrombophilias, asphyxial stress, dehydration, and an infection being more widespread in the neonate (Fitzgerald et al, 2006; Kenet et al, 2007). The use of anticoagulation therapy for the new child is predicated on case sequence and expert opinion however continues to be not determined. Recently, pointers regarding management, diagnostic analysis, and remedy were revealed by the American Heart Association Stroke Council (Roach et al, 2008). Hydration standing, monitoring and therapy of seizures, and antibiotics could also be important. In neonates with arterial ischemic stroke, anticoagulation may be thought-about in those with an ongoing cardioembolic source or recurrent stroke. Risk Factors A number of different varieties of research of infants with perinatal stroke has discovered an association with cardiac issues, blood problems, infection, trauma, medicine, maternal and placental issues, catheterization, extracorporeal membrane oxygenation, and perinatal asphyxia. In some research, the incidence of multiple risk factors has been famous, particularly blood disorders and asphyxial stress (Golomb et al, 2001; Lee et al, 2005). Perinatal trauma can result from various causes in utero, during labor, and postnatally. Mechanical trauma may cause harm to both cranial and extracranial constructions as nicely as the spinal cord and peripheral nerve buildings. Subgaleal Hemorrhage In sure cases the trauma may be extreme sufficient to cause a subgaleal hemorrhage, which consists of extension of the bleeding beneath the scalp aponeurosis to the nape of the neck. This condition needs to be recognized immediately because it can lead to severe blood loss and shock. The coagulation standing ought to be evaluated, because subgaleal hemorrhage could additionally be a presenting signal of hemophilia, hemorrhagic disease of the new child, or other coagulation problems. Maintenance of the circulatory standing of the toddler is crucial and may require use of packed cells or plasma to appropriate hypovolemia and any coagulopathy. Occasionally, severe trauma can result in tearing of both the tentorium or the falx cerebri. Mechanical Trauma Mechanical trauma may find yourself in injury to extracranial constructions, cranial structures, intracranial structures, spinal cord, or peripheral nerves. Molding of the Head and Caput Succedaneum Molding of the pinnacle is frequently seen in the new child delivered both vaginally or by cesarean section. It refers to the asymmetrical form of the pinnacle that outcomes from mechanical strain exerted during passage through the delivery canal or throughout extraction by cesarean section. Cephalohematoma Hemorrhage beneath the subperiosteum of the scalp leading to an elevation in usually the parietal area of the cranium is known as a cephalohematoma. It is seen twice as regularly in male infants and presents bilaterally in 15% of sufferers. Linear fractures are seen in 5% of unilateral lesions and in 18% of bilateral lesions. Resorption of the extravasated blood can lead to hyperbilirubinemia, and infants ought to be noticed for jaundice. Infection of the mass with formation of an abscess and associated osteomyelitis can occur in uncommon cases.
Generic 25mg persantine free shipping
Angiotensin-converting enzyme inhibitors are more practical in neonates because renal vascular resistance is high on this population; however medications janumet purchase 100mg persantine, if renal vascular illness is suspected symptoms bladder cancer persantine 25mg quality, this latter class of drugs ought to be avoided until normal vasculature is confirmed. In a hypertensive crisis, the drug of selection in this population is a calcium channel blocker-nicardipine. Other agents have additionally been used, similar to esmolol, labetalol, hydralazine, sodium nitroprusside, and enalapril. Intermittently administered intravenous agents, similar to hydralazine and labetalol, can be used in infants. Intravenous sodium nitroprusside, a potent vasodilator, acts quickly however has a short duration of action. Sodium nitroprusside can cause renal insufficiency or thiocyanate toxicity with larger than 72 hours of administration; therefore thiocyanate levels should be monitored with this drug whether it is used for a protracted interval. Enalaprilat, the intravenous angiotensin-converting enzyme inhibitor, has also been reported to be useful in the remedy of neonatal renovascular hypertension. This drug should be used cautiously because its use, even in doses on the lower finish of published ranges, can lead to significant and prolonged hypotension and oliguric acute renal failure (Flynn, 2000) (Table 88-2). Neonatal hypertension brought on by ureteral obstruction or aortic coarctation is greatest managed surgically. Monagle P, Chalmers E, Chan A, et al: Antithrombotic therapy in neonates and youngsters: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition), Chest 133(Suppl 6):887S-968S, 2008. Proesmans W, van de Wijdeven P, Van Geet C: Thrombophilia in neonatal renal venous and arterial thrombosis, Pediatr Nephrol 20:241-242, 2005. Hypertension ensuing from acute tubular necrosis resolves when renal operate improves, as is the case with other reversible causes. In bronchopulmonary dysplasia, if hypertension is because of steroid consumption (rarely used), it improves once the treatment is stopped. In hypertension secondary to renal artery or aortic thrombosis, the usual duration of drug therapy is a couple of weeks to a number of months. This chapter critiques a quantity of developmental themes, many of which are explored further in the following chapters in Endocrine Disorders and different parts of this textual content. In addition, classes discovered from growth of critical endocrine interactions and intracellular regulatory occasions, such because the endocrine pancreas (Puri and Hebrok, 2010), are being utilized to regenerative medication and modulating cell destiny determination within the adult. The placental-fetal unit sustains "the distinctive endocrine milieu of the fetus" (Fisher, 1986) and promotes adaptation for postnatal life. During fetal growth into the perinatal transition, the organism shifts from dependence on placenta to impartial homeostatic regulation. The useful development of fetal endocrine glands and hormonal responsiveness of goal tissues are influenced by fetal genotype, maternal genotype, maternal pre-pregnancy and pregnancy well being and diet, and pregnancyassociated and preexisting maternal circumstances. This advanced interplay of genotype and environment is emerging as a central thesis in translational analysis. By modifying placental and fetal growth and metabolism, hormones play a central role in programming growth in utero and adjusting phenotype, especially in response to antagonistic intrauterine situations (Fowden and Forhead, 2009). Of note, a lot understanding about endocrine developmental biology has been derived from giant animal fetal physiology fashions and gene manipulation in mice. When comparing ontogenic research carried out in different species, one should think about similarities and variations from human fetuses and newborns. Different species (and completely different organ systems in the same species) could also be classified either as immature (altricial) or more developed (precocial). A second precept is that the human fetal endocrine system begins growth roughly impartial from maternal endocrine influence. This separation is possible as a end result of the placenta is an environment friendly barrier to fetal entry to most maternal hormones, together with steroids, sterols, peptides, glycoproteins, and catechols. Nevertheless, transplacental passage of even minute amounts of a number of maternal hormones may be essential for regular fetal development. For instance, in human fetuses with congenital hypothyroidism (Chapter 93), maternal-fetal transfer of thyroid hormone (T4) could end in neonatal plasma levels 25% to 50% of these in regular newborns (Vulsma et al, 1989). Therefore, neurodevelopmental consequence in congenital hypothyroidism is generally good when T4 alternative is initiated throughout the first 2 weeks after delivery. In contrast, maternal hypothyroidism throughout being pregnant adversely affects neurodevelopmental outcome in the offspring (Haddow et al, 1999), and the mix of severe maternal and fetal hypothyroxinemia leads to profound neurodevelopmental disability (Yasuda et al, 1999). A third principle is that disturbances in transplacental substrate transfer-for instance, calcium (Chapter 90) or glucose (Chapter 94)-can modify improvement of fetal and neonatal hormonal pathways. Maternal immunoglobins and certain therapeutic agents also are transported to the fetus. Hesx1, a "grasp change" essential for normal optic nerve and pituitary development, orchestraties expression or activation of different elements involved in pituitary organogenesis (Corneli et al, 2008). At least 9 mutated pituitary transcription factors have been identified that alter hypothalamic-pituitary development and construction (Table 89-1). Proteins presently known to trigger fetal and neonatal nonneoplastic endocrine hyperfunction disrupt hormone exocytosis or cell sensing of an extracellular regulator of hormone exocytosis (Marx, 1999). A second important genetic mechanism for developmental endocrinopathies entails genomic imprinting. In mammals, some (imprinted) genes are expressed solely from either the paternally or maternally inherited allele. Maternal and paternal imprints are established, respectively, in dividing diplotene oocytes and prospermatogonia. Lack of imprinting of particular chromosomes or chromosome segments happens on account of uniparental disomy or deletions of imprinted facilities. Imprinting defects could cause distinct developmental abnormalities according to the chromosome concerned (Tilghman, 1999). The chief mechanism involves differential methylation of particular sites in or near imprinted genes. Maternal ldl cholesterol is the principal substrate for placental synthesis of progesterone precursors in fetal androgen production. In primates, estrogen performs an integrative role in modulating placental-fetal communication and in intrauterine growth (Albrecht and Pepe, 1999). Estrogen promotes placental trophoblast differentiation into syncytiotrophoblast and upregulates key enzymes in progesterone biosynthesis and cortisol-cortisone conversion. Throughout most of gestation, protection from hypercortisolism is crucial for normal neuroendocrine improvement. Studies on the role of glucocorticoids in preterm labor and fetal maturation have led to the successful, widespread use of antenatal glucocorticoids to accelerate fetal, especially lung, maturation (Liggins and Howie, 1972) (Chapter 42). This is a central mechanism for the fetus to exert an influence on being pregnant length. The increased fetal adrenal cortisol manufacturing and decreased placental cortisol clearance synchronize maturation of important organs (lung, liver, intestine, adrenal, brain). In effect, time period start may be viewed as an escape mechanism from this intrauterine surroundings of increasing hypercortisolemia. Positive suggestions loops are intrinsically unstable and, in this occasion, terminate in start.
Discount 100 mg persantine amex
Ampicillin and gentamicin provide excellent treatment for the most typical pathogens which might be likely to treatment viral pneumonia persantine 25 mg purchase with mastercard be present medicinenetcom generic persantine 100mg fast delivery. The period of intravenous antibiotic therapy for pyelonephritis could be debated, but parenteral therapy no much less than avoids the concern of compliance points. In view of given the expense of hospitalization or home-based intravenous antibiotic therapy, the mandatory length of parenteral therapy will proceed to be debated, especially in older youngsters (Hoberman and Wald, 1999). However, in the extra vulnerable neonate, parenteral remedy must be instituted in a hospital setting and continued until outcomes of a followup urine tradition become adverse (American Academy of Pediatrics, 1999). At that point, oral antibiotic therapy may be started for a complete course of 10 to 14 days. Once the acute an infection has been handled, antibiotic prophylaxis ought to be instituted until the kid is ready for radiographic imaging studies. In distinction, excessive doses of trimethoprim-sulfamethoxazole, and particularly of broadspectrum antibiotics, have been proven to produce higher and extra concerning shifts in fecal flora. A patient must be maintained on antimicrobial prophylaxis till imaging rules out any urinary tract pathology. On sonography, you will need to get hold of both kidney and bladder views, as a end result of typically the kidneys alone are imaged and proven to be normal and the workup is terminated; a quantity of infections later, a bladder ultrasound research exhibits a stone, ureterocele, or diverticulum. Because the act of voiding is required to show reflux in 20% to 30% of reflux cases, such instances could be missed if the child were anesthetized for a static cystogram. The normal strategy is to acquire a basic fluoroscopic study first, outline the anatomy, and precisely grade the reflux whether it is current. Understanding these research limitations is crucial before attempting to apply these standards to fragile neonates who usually have comorbidities. These principles are further illustrated in medical scenarios presented in this chapter. A great deal is thought concerning the bladder mucosal expression of these complex glycoproteins, with some being mannose-sensitive. Areas within the best kidney perform nicely and excrete contrast, whereas different lobes present indicators of poor perfusion. It used to be extremely common for obstructive uropathies to manifest after urosepsis had developed. With the widespread use of prenatal sonography, nevertheless, most neonates with an obstructive uropathy are identified at start, and antibiotic prophylaxis is initiated. However, a neonate should still exhibit urosepsis secondary to an obstructive uropathy. The presence of an obstruction produces a harmful combination of bacteria, urinary stasis, and a heat environment with a near-ideal culture broth. Keeping this risk in thoughts is important as a outcome of the administration may be altered by way of surgical drainage by both ureterostomy or percutaneous nephrostomy. Under these circumstances, an ultrasound examination to rule out obstruction is warranted. Urine manufacturing permits for some antibiotic to attain these bacteria, and a great response could additionally be seen if the patient receives treatment early in the center of an infection. The regular course of the ureter travels via the bladder wall and underneath the mucosal layer to create a flap valve mechanism, which prevents vesicoureteral reflux. Reflux caused by anatomic malposition of the ureteral insertion into the bladder is referred to as major reflux. In other sufferers, reflux happens secondary to will increase in bladder strain, a situation referred to as secondary reflux. For example, many patients with posterior urethral valves may have reflux that disappears once the valves are resected. Grading reflux allows physicians to talk findings rapidly and to perceive what the probabilities are for the pure decision of primary reflux. A and B, the ultrasound examination showed indicators of right hydronephrosis and hydroureter. After cutaneous diversion of this ectopic ureter, the toddler grew to become afebrile, and ureteral reimplantation was performed successfully 6 months later. The International Reflux Study used this grading scale, which relies on findings of a conventional fluoroscopic voiding cystourethrogram. By evaluating the findings intimately, a greater understanding of the severity, potential therapy modalities, and end result may be achieved and used for the profit of the affected person. Growing medical proof (Sillen et al, 1992, 1996a, 1996b) means that voiding pressures are dramatically increased in infants with reflux, particularly in boys. These research have proven that, even in regular males, voiding pressures are elevated within the neonatal interval and decline dramatically during the first 2 years of life. The information reveal that voiding pressures in boys with high-grade reflux are sometimes threefold to fourfold larger than these seen in older youngsters. In these boys, reflux usually resolves in a surprisingly short time frame, implying that the pressures drop with maturation of bladder perform. These clinical observations are supported by experimental findings suggesting that there are gender-related differences in bladder neck function. The key concept is that voiding pressures are elevated, particularly in male neonates with reflux, and that these pressures diminish over time. These observations have great bearing on how reflux resolution charges ought to be interpreted in newborns. Outcomes for reflux resolution in neonates have been studied more extensively over the previous 15 years (Sj�str�m et al, 2004); this was made potential by the elevated number of cases detected by prenatal ultrasonography. Evidence from a multicenter examine means that reflux detected in the first months of life as a part of a workup for prenatal hydronephrosis has a greater chance for spontaneous decision, grade for grade, than that identified within the youngster at 2 to four years of age (Herndon et al, 1999). This radiographic finding was also confirmed at cystoscopy, where the ectopic ureter (+) clearly enters the proximal urethra beneath the bladder neck (*). However, this course of action demands that parents comply with antibiotic prophylaxis and understand that a breakthrough infection price as excessive as 20% is feasible (Herndon et al, 1999). This sequence also indicated the good thing about circumcision in males with identified reflux (Herndon et al, 1999). A baby with innate susceptibility will still expertise bladder infections regardless of the absence of reflux. Several research have shown that siblings of sufferers with reflux even have a higher chance of having reflux, with an incidence that declines in older siblings. Several studies have shown an increased incidence of renal scarring in siblings whose reflux was found by screening (Sweeney et al, 2001; Wan et al, 1996). However, Parekh et al (2002) recommend that sibling reflux follows a more benign course, and so they famous no renal scarring after antibiotic prophylaxis. On the other hand, would the cohort of sufferers in this research have carried out as properly and not utilizing a prognosis and antibiotic prophylaxis In one metaanalysis of the world literature on screening research for reflux in asymptomatic siblings, Hollowell and Greenfield (2002) concluded that there was no proof to support this follow. The extent to which screening averts renal complications or hospital admissions for pyelonephritis shall be greatest answered by potential trials.
Best 100mg persantine
Chronic obstruction can result in medicine used to induce labor discount 25 mg persantine overnight delivery failure to thrive medications enlarged prostate persantine 100 mg purchase with mastercard, carbon dioxide retention, pulmonary hypertension, and ultimately right-sided heart failure (cor pulmonale). Feeding problems can be related to insufficient tongue management or pharyngeal hypotonia and sophisticated by presence of a cleft palate. However, estimates of start prevalence vary from 1:8500 to 1:20,000 births (Breugem and Mink van der Molen, 2009). Placement of a nasal trumpet or endotracheal tube may be required in an emergency, and it may be very important realize that extreme, life-threatening airway obstruction can current within the supply room. Though unusual, a prenatal prognosis of micrognathia allows for involvement of neonatologists and otolaryngologists in the supply room. Placing the child within the susceptible or lateral decubitus place will often open up the airway and reduce the degree of obstruction. This might improve airway patency and air trade, which decreases the work of respiratory and may improve tolerance of oral feeding. Tracheostomy could also be necessary to present a secure and secure airway in some infants. An endotracheal tube could be modified so that it can be passed by way of the nares into the hypopharynx above the epiglottis, permitting oxygenation/ventilation by bypassing the obstruction at the base of the tongue (Parhizkan et al, 2010). However, long-term follow-up signifies that many infants require secondary interventions to handle their feeding and airway and eventually their orthognathic points (Denny et al, 2004). For some neonates, mandibular distraction osteogenesis may be an different to tracheostomy. Recognition of different airway anomalies or issues, such as laryngotracheomalacia or subglottic stenosis, may also affect determination making relating to airway management. Nutrition can be maintained with a hypercaloric formula and/or fortified breast milk given by side-lying feeding using a cleft feeder, via nasogastric feeding tube, or via gastrostomy tube. As tone improves, the kid positive aspects higher management of the tongue, and development ensues, feeding will become less of an issue. Close remark for any symptoms of gastroesophageal reflux with proactive pharmacologic therapy can decrease airway inflammation. Given the affiliation with cognitive and motor delay, shut monitoring of growth and referral to early intervention providers, corresponding to a Birth to Three program, are recommended. One case of orofacial cleft occurs in approximately every 500 to 550 births, and on an average day in the United States, 20 infants are born with an orofacial cleft (Tolarova and Cervenka, 1998). The etiology of nonsyndromic clefts is complicated and multifactorial, likely ensuing from interaction between environmental and genetic components. Stickler syndrome is an autosomal dominant (with variable expressivity) connective tissue disorder with predominantly ophthalmic, orofacial, auditory, and articular manifestations and has been divided into three sorts (type 1 and a couple of have ocular findings, sort three is nonocular). Stickler syndrome is characterized by cleft palate, hearing loss, arthropathy, joint hypermobility, lowered top and eye abnormalities including myopia, cataracts, glaucoma and retinal detachment. The myopia of Stickler syndrome is often congenital, nonprogressive, and of high degree. F, Infant with Van der Woude syndrome with unilateral complete cleft lip and a lip pit (arrow). Clefts can have an effect on the first palate (lip, alveolus, or anterior portion of the hard palate that extends to the incisive foramen) and secondary palate (posterior onerous palate and soft palate). Clefts of the primary and secondary palate can be unilateral or bilateral and complete or incomplete. Children with cleft palate are at increased danger for eustachian tube dysfunction, recurrent otitis media, and bought listening to loss, in addition to speech points later in childhood. Feeding difficulties, nasal regurgitation of feeds, and difficulty gaining weight might occur in infants with a cleft palate (submucous and overt clefts of the palate). Lateral facial clefting or macrostomia is related to syndromes, including craniofacial microsomia and Treacher Collins syndrome. Midline clefting could be associated with different congenital defects as may be seen in orofaciodigital syndrome and frontonasal dysplasia. Clefting of the larynx may lead to stridor, a hoarse cry, respiratory misery, swallowing dysfunction, feeding difficulties, regurgitation, and aspiration. Endocrine abnormalities can come up because the midline malformation impacts the event of the hypothalamus and the pituitary gland. Clinical manifestations can embrace growth hormone deficiency, adrenal hypoplasia, hypogonadism, diabetes insipidus, and thyroid deficiency. Neurologic manifestations that warrant close attention include seizures, hypotonia, spasticity, autonomic dysfunction and developmental delays. An infant boy with hypertelorism, hypospadias, orofacial clefting, and symptoms of airway obstruction or aspiration ought to be evaluated for Opitz syndrome. Because of the potential influence of the orofacial cleft on respiratory, eating, hearing, speech, facial development, and dental well being, it is suggested that infants and children with clefts be referred to a multidisciplinary care team for long-term administration. In remote areas, the nearest cleft staff could also be found via the Cleft Palate Foundation web site. Box 95-1 outlines one instance of the multidisciplinary staff of suppliers that might contribute to the care of a kid born with a craniofacial malformation. On the preliminary evaluation, the supplier should assess the cleft and study the infant for dysmorphic features and different anomalies. A neonate with an entire cleft lip should be evaluated by a craniofacial or cleft staff within the first 2 weeks of life, and a few centers provide taping or presurgical molding (nasoalveolar molding) that can be initiated on this time interval. Many mothers will have the ability to breastfeed an toddler born with an isolated cleft lip. Thus, infants with cleft palate � cleft lip should be offered expressed breast milk or infant formulation using a specialized cleft feeder. There are a selection of cleft nipples/bottles which have been devised to allow for oral feeding together with the cleft palate nurser (squeeze bottle), Haberman feeder, and Pigeon bottle ( Make certain the kid is feeding in an upright place, as gravity will assist prevent nasal regurgitation. Adequate weight achieve is essential, as a end result of these children will bear a number of surgeries in the 1st year of life. Newborns with clefts are thought of nutritionally excessive risk, and a dietitian must be consulted to assist determine caloric wants and to carefully monitor growth. In common, surgical closure of the lip and nasal deformity is done within the first three to 6 months of life. Palatoplasty sometimes occurs between 9 and 12 months of age to optimize speech and language improvement. If there are concerns about airway clefting or anomalies of the larynx or trachea, a chest x-ray must be obtained and the airway evaluated, in addition to applicable analysis of related anomalies. Microlaryngoscopy under common anesthesia remains the gold commonplace in the diagnosis of a laryngeal cleft (Rahbar et al, 2006). Early prognosis and proper restore of the laryngeal cleft are essential to forestall harm to the lungs. In approaching diagnosis of a syndrome, it is important to categorize the sort of cleft (lip with or with out palate, U-shaped or V-shaped cleft palate, or more atypical orofacial cleft) and to look for some other malformations. A referral to a medical geneticist is beneficial when an underlying diagnosis is suspected but not established.