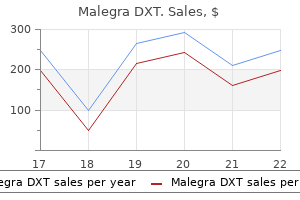
Cheap malegra dxt 130 mg
The veins accompanying the other arteries of the lower limb are within the nature of venae comitantes erectile dysfunction pills in pakistan purchase malegra dxt 130 mg overnight delivery. The dorsal and plantar surfaces of the foot are coated by subcutaneous venous plexuses erectile dysfunction at age 33 buy malegra dxt 130 mg lowest price. Along the edges of the foot, there are medial and lateral marginal veins that talk with each the plantar and dorsal venous networks. The great (or long) saphenous vein is a continuation of the medial marginal vein of the foot. It ascends into the leg, somewhat in entrance of the medial malleolus and lies for far on the medial surface of the tibia. In the higher a half of the thigh, it passes considerably laterally and passes through an aperture within the deep fascia (saphenous opening) to finish in the femoral vein (10. The nice saphenous vein receives numerous tributaries from the entrance the foot and again of the leg, and from the entrance of the thigh. It also receives the anterior cutaneous vein of the thigh which drains the lower part of the front of the thigh. Just below the knee it receives the anterior vein of the leg, and the posterior arch vein. Over the dorsum of the foot the nice saphenous vein receives the medial marginal vein of the foot. The great saphenous vein is linked to the deep veins of the leg and thigh by way of a variety of perforating veins which are talked about under. The small (or short) saphenous vein is a continuation of the lateral marginal vein of the foot. It ascends behind the lateral malleolus, and runs upwards along the center of the back of the leg. Over the lower part of the popliteal fossa, it perforates the deep fascia and ends in the popliteal vein, a number of centimeters above the knee joint (10. The perforating veins (or perforators) are so called, as they perforate via the deep fascia. Similar communications with deep veins exist where the great and small saphenous veins finish in deep veins. A perforator that connects the great saphenous vein to the femoral vein is present in the decrease part of the adductor canal (Number 1). A perforator current just below the knee connects the nice saphenous vein, or the posterior arch vein, with the posterior tibial vein (Number 2). There are a selection of perforators in the lower one third of the leg (number 4, 5, 6). Venous Return from the Lower Limb Venous blood from the lower limbs has to ascend to the guts in opposition to gravity. When muscular tissues contract, they enhance in thickness elevating the strain within the sleeve. In this way, muscular contraction acts as a pump that helps in venous return from the lower limbs. The upper superficial inguinal lymph nodes lie along the inguinal ligament, instantly under the latter. Note that in addition to the decrease limb these nodes drain constructions in the perineum, and the stomach wall beneath the level of the umbilicus. The pores and skin of the lateral aspect and back of the leg is drained by vessels which run along the short saphenous vein and end in the popliteal lymph nodes, from the place the lymph passes through deeply positioned lymph vessels to the deep inguinal nodes. Some deep vessels of the gluteal area run along the superior and inferior gluteal vessels to finish in nodes along the internal iliac vessels. Infection in any part of the lower limb may find yourself in enlargement and tenderness of the inguinal lymph nodes. It has to be remembered that in addition to the lower limb, the inguinal nodes drain the lower a part of the abdominal wall (up to the extent of the umbilicus). They additionally drain the perineum together with the decrease components of the anal canal, the vagina, and the urethra. The ligament is attached at its lateral end to the anterior superior iliac spine, and at its medial finish to the pubic tubercle. The ligament is really the folded decrease fringe of the aponeurosis of a muscle of the belly wall referred to as the exterior indirect muscle. The deep fascia of the thigh is connected to the ligament, and because of the pull of this fascia the ligament has a delicate downward convexity. It is seen to emerge through an aperture in the abdominal wall located simply above the medial finish of the inguinal ligament. A little below the medial end of the inguinal ligament, we see the saphenous opening. On the medial aspect, the fascia forming the boundary of the saphenous opening merges with the fascia over a muscle referred to as the pectineus. The saphenous opening is closed by a sheet of fascia which has many small holes in it. The saphenous vein curves round the lower margin of the saphenous opening, and pierces the cribriform fascia to end by joining the femoral vein. The cribriform fascia is also penetrated by three small branches of the femoral artery. These are the superficial circumflex iliac artery (laterally), the superficial epigastric artery (in the middle) and the superficial external pudendal artery (on the medial side). Veins accompanying these three arteries normally end in the terminal a half of the saphenous vein before the latter pierces the cribriform fascia. The fascia within the perineum is immediately steady (over the pubic symphysis) with the corresponding fascia over the abdominal wall. When traced superiorly, its gains attachment to bones and ligaments that lie at the upper restrict of the upper limb. Along the lateral margin of the thigh, the fascia lata is thickened and types a powerful band passing from the anterior a half of the iliac crest to the upper end of the tibia (front of lateral condyle). At its higher finish, the tract splits to enclose a muscle known as the tensor fasciae latae. The thickness of the deep fascia in the region of the iliotibial tract is due to the pull of those muscle tissue. The iliotibial tract helps to transmit the pull of these muscular tissues to the tibia and helps to stabilize the knee. The space of attachment of the iliotibial tract to the tibia varieties a outstanding triangular impression on the bone (9. Intermuscular septa (lateral, medial and posterior) passing from deep fascia to the femur assist to divide the thigh into anterior, medial and posterior compartments. Preliminary Identification of Muscles seen on the Front and Medial Side of the Thigh the muscles to be seen on the front and medial facet of the thigh after elimination of deep fascia are proven in 10. Its upper finish is hooked up to the anterior superior iliac spine, whereas its decrease end (insertion) reaches the medial side of the higher end of the tibia. Running downwards alongside the lateral margin of the upper part of the thigh we see the tensor fasciae latae and the iliotibial tract (already talked about above).
Malegra dxt 130 mg buy mastercard
Starting behind the corresponding sternoclavicular joint each artery runs upwards and considerably laterally up to causes of erectile dysfunction in 40 year old malegra dxt 130 mg cheap fast delivery the level of the upper border of the thyroid cartilage (42 erectile dysfunction cream 130 mg malegra dxt order with mastercard. In its upward course, every frequent carotid artery lies in a triangular space bounded: a. The artery is enclosed in a fibrous carotid sheath that also encloses the interior jugular vein (lateral to the artery) and the vagus nerve (lying posterior to the interval between the artery and the vein). The inferior thyroid artery runs transversely behind the lower a part of the artery (42. On the right side only, the artery is crossed posteriorly by the recurrent laryngeal nerve; and on the left facet only, by the thoracic duct. Apart from the sternocleidomastoid muscle the buildings masking the artery anterolaterally are: a. The sternohyoid and sternothyroid muscles (in its lower part, deep to the sternocleidomastoid) b. The superior stomach of the omohyoid muscle (at the extent of the cricoid cartilage) ii. The sternomastoid department of the superior thyroid artery (above the omohyoid) 834 Part 5 Head and Neck Relationship of frequent carotid artery to the larynx, trachea and thyroid. Some constructions deep to the artery are also proven Right lateral view showing constructions crossing superficial to the widespread carotid artery iii. The recurrent laryngeal nerve (running vertically between the trachea and the oesophagus) b. The internal carotid artery begins at the upper border of the thyroid cartilage and ascends to attain the bottom of the cranium where it enters the carotid canal. Each artery could also be thought of as the principle upward continuation of the common carotid artery and occupies an identical position (Compare 42. It lies on the transverse processes of the upper cervical vertebrae being separated from them by the longus capitis and the superior cervical sympathetic ganglion. Superficially, the artery is crossed by numerous buildings which would possibly be listed in 42. On reaching the bottom of the cranium, the artery enters the petrous a part of the temporal bone via the external opening of the carotid canal. It now undergoes a second bend to run vertically by way of the higher a part of this foramen to enter the cranial cavity. Here, it undergoes a 3rd bend to run forwards on the facet of the physique of the sphenoid bone. Near the anterior finish of the physique of the sphenoid bone it again bends upwards (fourth bend) on the medial side of the anterior clinoid course of. Here, it pierces by way of the dura mater forming the roof of the cavernous sinus and comes into relationship with the cerebrum. The artery now turns backwards (fifth bend) to reach the anterior perforated substance of the brain. The artery terminates here by dividing into the anterior and middle cerebral arteries. Throughout its course the artery is surrounded by a plexus of sympathetic nerves derived from the superior cervical sympathetic ganglion, and by a plexus of veins that join the intracranial veins to those outdoors the cranium. As it lies within the carotid canal, the artery is intently related to the center ear, the auditory tube and the cochlea. The artery has a extra intimate relationship with the abducent nerve that runs in shut contact with the inferolateral side of the artery. After piercing the dura mater, the artery has the optic nerve above it and the oculomotor nerve below it. The cerebral arteries shall be thought-about within the section on the mind (Chapter 56). In addition to these, the interior carotid artery gives off a quantity of smaller branches which are proven in 42. The posterior speaking and the anterior choroidal artery are intimated related to the brain and might be described in Chapter fifty six. The ophthalmic artery passes forwards to enter the cavity of the orbit by way of the optic canal. Coronal part by way of the cavernous sinus showing the interior carotid artery and associated structures Chapter 42 Blood Vessels of Head and Neck 837 Scheme to present the branches given off by the internal carotid artery 2. It pierces the dural sheath of the nerve and runs forwards for a brief distance between these two. Just near its origin from the ophthalmic artery, the lacrimal artery gives off a recurrent meningeal department that runs backwards to enter the middle cranial fossa by way of the superior orbital fissure. The lacrimal artery provides off two zygomatic branches that enter canals within the zygomatic bone. Their terminal branches (specially of the anterior artery) enter the nose and supply part of it. The supratrochlear artery is probably certainly one of the terminal branches of the ophthalmic artery. Each exterior carotid artery arises from the frequent carotid at the stage of the upper border of the thyroid cartilage (or the level of the disc between the third and fourth cervical vertebrae) (42. From its origin, the artery runs upwards and terminates behind the neck of the mandible. Scheme to show the branches of the ophthalmic artery Chapter 42 Blood Vessels of Head and Neck 839 Course of central artery of retina Scheme to show the landmarks to which the exterior carotid artery, and its branches, are related. Above the triangle, the artery lies deep to the posterior stomach of the digastric muscle and the parotid gland. The pharynx is separated from the higher a part of the artery by the styloid process (and some muscle tissue attached to it) and by the inner carotid artery. In addition to the relations mentioned above the exterior carotid artery is crossed by several buildings that move superficial or deep to it. The branches of the external carotid artery and their levels of origin are as follows (in order of origin) (42. The ascending pharyngeal artery arises from the deep aspect of the external carotid artery simply above its decrease finish. The superior thyroid artery arises from the front of the external carotid slightly below the level of the larger cornu of the hyoid bone. The lingual artery arises from the entrance of the exterior carotid artery reverse the tip of the larger cornu of the hyoid bone. The facial artery arises from the front of the external carotid a little above the origin of the lingual artery. The occipital artery arises from the back of the external carotid reverse the origin of the facial artery. The posterior auricular artery arises from the back of the external carotid just above the extent at which the latter is crossed by the posterior stomach of the digastric muscle. The superficial temporal artery and the maxillary artery are terminal branches of the exterior carotid artery. They begin behind the neck of the mandible, in the substance of the parotid gland. The ascending pharyngeal artery runs upwards to the base of the skull, lying between the pharynx and the inner carotid artery.
130 mg malegra dxt order mastercard
Neck node metastases are quite common from major sites inside the hypopharynx icd 9 code erectile dysfunction due diabetes purchase malegra dxt 130 mg with amex, with the piriform fossa having the highest incidence erectile dysfunction facts cheap malegra dxt 130 mg with mastercard. Postcricoid tumours could metastasize to the mediastinal and paratracheal group of nodes, in addition to nodes in the neck. This was noted in thyrotoxic patients who have been handled by localized radiotherapy to the neck earlier than the development of drug remedy. Treatment of sideropenic dysphagia is directed towards correcting the haematological deficits by administration of iron and generally vitamin B advanced. Paterson�Brown Kelly syndrome There is a recognized association between sideropenic dysphagia and postcricoid carcinoma. Paterson and Brown Kelly described a syndrome (also known as Plummer�Vinson) comprising hypochromic microcytic anaemia, glossitis, koilonychia, splenomegaly and a postcricoid net with dysphagia. Haematological abnormalities embrace a low serum iron and a raised whole iron binding capability. Initially, the one criticism may be odynophagia (pain or discomfort on swallowing) or a sense of soreness and pricking as meals passes by way of the pharyngo-oesophagus. At the time of presentation, the dysphagia is normally severe and Hypopharyngeal carcinoma Aetiological elements Tobacco smoke and alcohol have been implicated in hypopharyngeal Hyoid bone 1 Posterior pharyngeal wall 2 Piriform sinus Cricoid 3 Postcricoid region. A microcytic anaemia is associated with (a) koilonychia, (b) glossitis and postcricoid net. Dysphonia results from both direct invasion of the larynx or vocal cord paralysis brought on by involvement of the recurrent laryngeal nerve. A unfavorable swallow within the presence of persistent feeling of one thing in the throat requires a formal pharyngo-oesophagoscopy. Dysphagia and weight reduction Prognosis the 5-year survival rates are about 15% with radiotherapy alone, but 30% general for all forms of remedy. The earliest symptom of hypopharyngeal neoplasia may merely be the feeling of something in the throat. The swallowing tube is greatest reconstructed using some form of visceral interposition. Nasopharyngeal carcinoma is the most common malignant tumour encountered, and the angiofibroma is the one benign tumour of any nice importance. The viral genome seems to turn into included into nasopharyngeal mucosal cells which may then be triggered by some stimulant to initiate malignant change inside the cell. Clinical features the majority of tumours arise in the fossa of Rosenm�ller and can unfold in any course to produce an unlimited array of potential symptoms and signs. The involvement of the trigeminal nerve by superior extension into the foramen ovale manifests as facial pain and altered sensation in the face. Invasion of the nasopharyngeal end of the Eustachian tube will give rise to otological symptoms such as hearing loss. Investigations the neoplasm may be seen on routine postnasal house mirror examination. All other patients ought to be subjected to formal biopsy under common anaesthesia. The radiotherapy is given to the nasopharynx and neck, even in the absence of palpable neck nodes. For recurrent disease in the nasopharynx or neck, additional chemotherapy and reirradiation is given. The proportion of each factor of endothelial vascular or fibrous connective tissue may be very variable. Clinical features Nasal obstruction and epistaxis are the most typical presenting symptoms. The mass is instantly seen with an indirect mirror, rigid endoscope or flexible rhinolaryngoscope. Angiographic assessment will also allow an opportunity to perform preoperative embolization to reduce the vascularity of the tumour and, therefore, minimize blood loss throughout any subsequent surgical removing. Cytotoxic remedy with or with out radiotherapy is used to control systemic lymphoma, and radiotherapy is used alone in localized disease. It can expand from its craniocervical site of origin into the nasopharynx and the neighbouring clivus and cervical vertebrae. They could be cauterized, but any recurrence ought to be excised and subjected to histological examination to exclude squamous cell carcinoma. The lesion is extra successfully excised by a lateral rhinotomy or midface degloving method. About 10% of the benign transitional cell lesions are associated with squamous carcinoma. Antral tumours normally current late, as the mass must develop to fill the sinus area before inflicting any major signs. Trismus (reduced jaw opening) is an indication that the pterygoid muscles have been invaded by direct posterior extension. Malignant tumours Aetiology Smoking is crucial danger factor for nasal most cancers. Hardwood dust is a recognized issue in the improvement of adenocarcinoma of the ethmoid sinuses. Investigations Histological affirmation of the malignant process is usually easy owing to the presence of a mass in the nasal cavity. The Ocular Proptosis Epiphora Diplopia Nasal Discharge (bloody and offensive) Obstruction Anosmia Mouth Loose enamel Ill fitting dentures Palatal swelling Miscellaneous Retroantral unfold inflicting trismus and alteration in facial sensation as a end result of V nerve involvement Clinical features Clinical options are depending on the exact location of the malignant tumour. For example, frontal sinus most cancers is more probably to cause orbital symptoms early within the illness. Neoplasia of the nose and paranasal sinuses superior extension of the disease into the region of the cribriform plate could also be included in the resection by performing a craniofacial resection, i. Management is difficult owing to late presentation, complex anatomy and the proximity of essential constructions such because the orbit and cranial contents. Management the management of malignant illness of the nose and paranasal sinuses depends on the histology and the extent of the neoplasm. The majority of instances require full-dose radiotherapy with subsequent deliberate surgical procedure. Palliative therapy is extraordinarily useful, as with out some form of therapy the illness is slowly progressive and cosmetically mutilating. Most malignant disease in the nostril and paranasal sinuses could also be resected through the lateral rhinotomy method or by performing a maxillectomy. Symptoms and signs could additionally be predominantly nasal, dental, orbital, facial or retroantral relying on the location and course of unfold of malignant disease. Extension of disease into the cribriform plate and anterior cranial fossa can be resected by using a cranial method in combination with the facial route (cf. The majority of parotid tumours are benign, but the incidence of malignancy is high at the different websites.
Cheap malegra dxt 130 mg overnight delivery
The original ventral floor of the limb is represented by the inguinal region zyprexa impotence order malegra dxt 130 mg amex, the medial side of the decrease a part of the thigh erectile dysfunction protocol download free cheap 130 mg malegra dxt amex, the popliteal floor of the knee, the again of the leg, and the sole of the foot. Anomalies of limbs the anomalies of the upper and decrease limbs are similar and will subsequently be thought-about together. One or more limbs of the physique could also be partially, or completely, absent (phocomelia, amelia). Absence of limb bones, in entire or partially, may also occur independently and could additionally be the cause for deformities of the limb. A digit could also be abnormally giant (macrodactyly) or abnormally brief (brachydactyly). As a rule, the arrangement of dermatomes is simple over the trunk, as successive horizontal strips of pores and skin are provided by every spinal nerve of the area. The skin of the upper part of the pectoral area is provided by spinal segments C3 and C4 (upto the extent of the sternal angle). The limb has developed from the area of the trunk provided by segments C5 to T1. The supraclavicular nerves (C3, 4) come up within the neck from the cervical plexus (as one ramus). The nerve trunk runs downwards and backwards deep to this muscle and appears at its posterior border. These branches descend over the posterior triangle of the neck giving some branches to the skin here. The medial supraclavicular nerve provides the skin of the upper and medial part of the thorax. The intermediate supraclavicular nerve provides the pores and skin over the higher a half of the pectoralis major. The area of provide of the medial and intermediate supraclavicular nerves extends as much as the level of the second rib. Skin under the level of the sternal angle is supplied by anterior cutaneous branches of the 2nd to sixth intercostal nerves. We additionally see two different muscle tissue components of that are seen within the region and are described right here. Along with the latter it forms a partition that separates the upper a part of the pectoralis main from the contents of the axilla. At the medial fringe of the pectoralis minor it splits to enclose the pectoralis minor. At the decrease (lateral) edge of the pectoralis minor the fascia turns into steady with the axillary fascia (formingthedome-shapedflooroftheaxilla). When traced medially, the fascia reaches the primary and second ribs and the higher two intercostal areas. Some lymphatics of the breast and pectoral area passing to the apical lymph nodes of the axilla also cross by way of it. The muscle is in entrance of the pectoralis minor, the clavipectoral fascia, and upper components of biceps brachii, the coracobrachialis and serratus anterior Insertion Nerve supply Action Notes three. Keeps medial finish of clavicle pressed towards articular disc of sternoclavicular joint, and smoothens actions 3. The platysma arises from the deep fascia over the upper part of the pectoralis major and the anterior part of the deltoid. The muscle is examined by making the patient place his palms against a wall and pushing towards it. If the muscle is paralysed the medial margin of the scapula is lifted off from the ribs. The anterior wall is shaped by the pectoralis major, the pectoralis minor and the clavipectoral fascia. Note that the latissimus dorsi winds round the decrease margin of the teres major, the two collectively form the thick posterior fold of the axilla. The lateral wall is formed by the humerus within the area of the intertubercular sulcus. The axillary fascia has an aperture via which the axillary tail of the breast enters the axilla. The apex of the axilla faces upwards and somewhat medially and lies on the degree of the outer border of the firstrib. These three structures type the boundaries of a gap by way of which the axillary vessels and the brachial plexus cross from the neck into the axilla. The contents of the axilla are the axillary artery and vein, and the axillary lymph nodes. The second half and the upper portion of the third part of the artery lie on the subscapularis muscle. The lower portion of the third half lies on the teres major muscle and the tendon of the latissimus dorsi. The entire artery (except its lowermost part) is overlapped by the pectoralis major. The axillary artery is accompanied by the axillary vein: the vein lies anteromedial to the artery (3. The third part of the artery is crossed anteriorly by the medial root of the median nerve as the latter passes laterally to be a part of the lateral root. The thoracoacromial artery arises from the second a half of the axillary artery deep to the medial margin of the pectoralisminor. The pectoral department descends between the pectoral muscles, supplying them and the chest wall. The clavicular branch runs upwards to supply the subclavius and the sternoclavicular joint. The deltoid branch runs laterally within the groove between the deltoid and the pectoralis major. The lateral thoracic artery runs downwards near the lateral margin of the pectoralis minor supplying pectoral muscular tissues, the serratus anterior and the axillary lymph nodes. The subscapular artery runs downwards along the lateral border of the scapula supplying muscles in the area and anastomosing with numerous different arteries. This branch winds around the lateral border of the scapula passing backwards via the triangular space. It offers branches to muscle tissue on both the ventral and dorsal aspects of the scapula. The anterior circumflex humeral artery runs laterally in entrance of the surgical neck of the humerus. It provides off a branch that ascends within the intertubercular sulcus to the shoulder joint. The posterior circumflex humeral artery runs backwards (accompanied by the axillary nerve) by way of the quadrangular space. It provides off a descending branch that anastomoses with a department of the profunda brachii artery. To stop bleeding, strain may be utilized over the axillary artery close to its lower finish. Pressure is utilized laterally, at a level simply above the decrease border of the posterior fold of the axilla.
Buy discount malegra dxt 130 mg
Liver tissue could be damaged by infections and by toxic substances reaching it by way of the bloodstream erectile dysfunction other names discount 130 mg malegra dxt fast delivery. All substances absorbed into the bloodstream from the gut cross erectile dysfunction causes young males 130 mg malegra dxt with amex, by way of the portal vein, into the liver. In individuals who devour excessive quantities of alcohol over long intervals, the liver tissue undergoes fibrosis (cirrhosis of liver). The liver tissue has considerable reserve and continues to carry out its regular features even after large amounts of it are broken. Tumours of the liver might come up either from liver cells or from cells lining bile capillaries. The liver is also a common site for secondary growths (metastases) brought on by malignancy elsewhere within the body. The proper and left, hepatic ducts emerge on the porta hepatis and join to kind the widespread hepatic duct. At its lower end, the common hepatic duct is joined by the cystic duct from the gall bladder to type the bile duct. The gall bladder is a small sac hooked up to the visceral floor of the liver (28. It is held in place by peritoneum that covers its inferior (or posterior) surface (28. The lowest a half of the gall bladder, which is known as the fundus, projects past the inferior border of the liver (28. The neck is linked to the cystic duct by way of which the gall bladder drains into the bile duct. The fundus is available in contact with the anterior abdominal wall slightly below the ninth costal cartilage. The space of contact corresponds to the point where the lateral margin of the proper rectus abdominis muscle crosses the costal margin. The mucous membrane lining the neck of the gall bladder is folded in a spiral method forming the so-called spiral valve. Some of those enter liver tissue instantly, while others be a part of veins draining the bile duct and in the end drain into the portal vein. The bile duct extends from slightly below the porta hepatis to the middle of the descending a half of the duodenum. Within the lesser omentum, the duct lies to the best of the hepatic artery and in entrance of the portal vein (28. The bile and pancreatic ducts could open separately on the main duodenal papilla, or may join (at a variable distance above the papilla) to kind a common passage called the hepatopancreatic ampulla. The bile duct is provided by branches from the hepatic, cystic and superior pancreaticoduodenal arteries (Chapter 29). Lymphatics from the gall bladder and bile duct drain to hepatic nodes (including cystic node) and coeliac nodes. The terminal a part of the bile duct is surrounded (just above its junction with the pancreatic duct) by a ring of smooth muscle that types the sphincter choledochus (choledochus = bile duct) (28. As a end result, bile shaped in the liver retains accumulating in the gall bladder (and also undergoes appreciable concentration). When food enters the duodenum (especially a fatty meal) the sphincter opens and bile stored in the gall bladder is poured into the duodenum. The sphincter choledochus is, due to this fact, important for filling of the gall bladder. Another less developed sphincter is often (but not always) present across the terminal part of the pancreatic duct. A third sphincter surrounds the hepatopancreatic ampulla and is known as the sphincter ampullae. The sphincter ampullae might extend upwards to enclose the lower elements of the bile and pancreatic ducts. The sphincters named above are often referred to collectively as the sphincter of Oddi (although this term strictly applies solely to the sphincter ampullae). CliniCal Correlation Clinical Correlation of Gall bladder and biliary Ducts Oral Cholecystography 1. The fundus of the gall bladder may be folded on itself to form a cap like structure called the phrygian cap. In the situation referred to as floating gall bladder, the gall bladder is lined by peritoneum on all sides. Instead of mendacity in its normal place the gall bladder might lie transversely beneath the right lobe, or may lie under the left lobe of the liver. The gall bladder might open instantly into the bile duct (sessile bladder), the cystic duct being missing. Agenesis, atresia, or duplication might affect the gall bladder or one of many ducts. It may join the widespread hepatic duct on its left side (instead of the traditional proper side). Sometimes, the cystic duct is very long and descends anterior to the duodenum earlier than joining the frequent hepatic duct. Chronic cholecystitis is usually related to the formation of stones within the gall bladder (cholelithiasis). The ache may radiate to the best scapula or right shoulder especially if the subdiaphragmatic parietal peritoneum is concerned. To take a look at for gall bladder irritation, the doctor locations a finger over the location where the proper costal margin meets the linea semilunaris (or on the tip of the ninth costal cartilage) and asks the affected person to take a deep breath. When a gall stone tries to move by way of the bile duct it causes severe ache known as biliary colic which is felt within the epigastrium. Obstruction to the biliary duct system from any cause results in the event of jaundice. In many circumstances, the bile and pancreatic ducts retain separate lumens right as a lot as the tip of the main duodenal papilla. When this widespread duct is lengthy, obstruction close to the orifice (by a calculus, or by spasm of muscle) can result in regurgitation of bile into the pancreatic duct. The wall of the gall bladder could turn into adherent to that of the duodenum and erosion right here might result in the formation of a fistula between the 2. A radiological method for investigation of the gall bladder (cholecystography) is described above. It lies obliquely on the posterior abdominal wall, partly to the best of the median plane and partly to the left. The neck is placed behind the pylorus and the physique of the pancreas lies behind the body of the stomach. The tail lies within the lienorenal ligament and its tip is out there in contact with the spleen. A projection arising from the decrease left part of the head is called the uncinate process of the pancreas (28. The anterior and posterior surfaces at the superior border and the inferior and posterior surfaces meet on the inferior border. A part of the body of the pancreas projects upwards past the lesser curvature of the stomach and comes in contact with the lesser omentum.
LPC (Propionyl-L-Carnitine). Malegra DXT.
- Poor circulation that causes leg pain while walking (intermittent claudication).
- Treating symptoms of age-related testosterone deficiency ("male menopause").
- What other names is Propionyl-l-carnitine known by?
- Dosing considerations for Propionyl-l-carnitine.
- A type of heart disease called chronic ischemic heart disease.
- Erection problems in men with diabetes.
- Are there any interactions with medications?
- Chronic fatigue syndrome (CFS), circulatory problems caused by diabetes, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96780
Discount 130 mg malegra dxt amex
Direct immunofluorescence of mucosa affected by erythema multiforme might show perivascular C3 deposits erectile dysfunction and urologist malegra dxt 130 mg cheap visa. Pemphigus demonstrates immune advanced deposits on the intercellular surfaces within the epithelial layer erectile dysfunction caused by zoloft buy malegra dxt 130 mg mastercard. A finding of immune complex deposits along the basement membrane is attribute of pemphigoid. Median rhomboid glossitis is an oval-shaped space of atrophy of floor papilla within the heart of the dorsal floor of the tongue, and is often asymptomatic. Lichen planus might present as clean plaques on the tongue, and will come and go, giving a picture much like erythema migrans (geographic tongue). However lesions of geographic tongue are typically properly outlined and bordered by a definite irregular white line. Overgrowth and subsequent staining of filiform papillae on the dorsal floor of the tongue ends in black hairy tongue. Which of the following situations could additionally be seen in a affected person with an accentuated linea alba A 25-year-old male with a number of jaw osteomas, epidermoid cysts and a number of supernumerary tooth ought to bear which of the next: A. Leukoedema appears grayish white, typically affecting the buccal mucosa bilaterally. There could additionally be wrinkles or striations present, however these disappear when the mucosa is stretched. Hairy leukoplakia appears as a shaggy white masking of the mucosa, usually on the lateral facet of the tongue. The first three lesions might appear remarkably comparable on inspection, and may only be distinguishable histologically. Epulis fissuratum usually seems on the margin of an ill-fitting denture, and could additionally be grooved by it. It represents the region of friction on the buccal mucosa comparable to the occlusal line of the tooth. However a markedly accentuated line could additionally be seen in sufferers who habitually clench or grind their enamel. Intestinal polyps are extraordinarily frequent in such patients, and colonoscopy is warranted to display for malignancy since their rate of malignant transformation is so high. Multiple visceral and cutaneous granular cell tumors: ultrastructural and immunocytochemical proof of Schwann cell origin. Other variants: onset in early childhood � Non-healing groin rash widespread: papules, pustules, vesicles turn out to be crusted and impetigenized. A mother brings her 3-month-old infant to your office for analysis of a rash within the diaper space. On biopsy you see large mononuclear cells with reniform nuclei scattered in the dermis. He typically notices blood on his underwear that he attributes to scratching these lesions. This is a description of diaper dermatitis attributable to the urine and stool in areas of contact. Long-term use of topical super-potent steroids might lead to atrophy and cause skin breakdown however the query said she used them intermittently. A 55-year-old female with lichen sclerosis of the vagina and perineum has been well-controlled with topical clobetasol propionate ointment intermittently for the last 10 years. A 40-year-old man presents with a number of, small, red-brown papules with a flat-to-verrucous floor on the shaft of his penis. A 25-year-old medical student involves your workplace as a end result of he notes an space of hyperpigmentation on the glans penis. The lesion will begin out more erythematous but seems to wax and wane and at times is kind of completely resolved. He is otherwise healthy aside from seasonal allergies for which he takes an over-the-counter medication to treat as wanted. A 17-year-old feminine presents to your workplace with a model new pruritic rash involving her axillae, inguinal area, and posterior neck. A lichenoid infiltrate in a band-like distribution which obscures the dermoepidermal junction C. Atypical cells with pale-staining cytoplasm and atypical nuclei, mitoses distributed singly or in clusters within the epithelium 6. This is a typical scenario for a hard and fast drug response related to pseudoephedrine, a standard ingredient in cold and allergy medication. It is autosomal dominant and on pathology is described as the "dilapidated brick wall. Shaving is the remedy of choice for trichomycosis axillaris which might affect the pubic hair. Damsted Petersen C, Lundvall L, Kristensen E, Giraldi A: Vulvodynia: definition, diagnosis and remedy. Shah V, Shet T: Scrotal calcinosis results from calcification of cysts derived from hair follicles: a collection of 20 instances evaluating the spectrum of changes resulting in scrotal calcinosis. Subsequent publicity to the allergen will end in incrementally more extreme reactions � Common allergens include: crops from the Toxicodendron genus. Balsam of Peru (also referred to as Myroxylon pereirae) � Wood extract derived from Myroxolon balsamum tree � Contains � Cinnamein (cinnamic acid, cinnamyl cinnamate, benzyl benzoate, benzoic acid and vanillin) 9. Constituents: -amylcinnamic alcohol, cinnamic alcohol, cinnamic aldehyde, eugenol, geraniol, hydroxycitronellal, isoeugenol, oak moss absolute � Along with balsam of Peru, Fragrance Mix I detects the majority of sufferers with a fragrance allergy 10. Ammonia persulfate � Peroxide hair bleaches � Bleached baking flour � Contact urticaria and anaphylactoid reactions 4. Cocamidopropyl betaine � Allergen may be dimethylaminopropylamine or amidoamine (residues from synthesis) � Surfactant � Shampoo (dermatitis in hair dressers), liquid soaps Embalming fluid, electron microscopy, cosmetics, waterless hand cleansers, wallpaper, liquid fabric softener, leather-based tanning 5. Ethylenediamine dichloride � Stabilizer in topical lotions, medicines, dyes, rubber, resin, waxes, pesticides, asphalt, fungicides � Previously found in nystatin cream � Cross-reacts with aminophylline, antihistamines (hydroxyzine), meclizine (antivert) four. Ethyl cyanoacrylate � Instant glue ("Super Glue"), synthetic nail glue � Liquid bandages, sealant for ileostomy appliances � Electronic circuit boards, aircrafts, cars 2. Methyl methacrylate � Clear, inflexible plastic (artificial nails, exhausting contact lenses, listening to aids, dentures, dental fillings/ sealants) � Glue for surgical prostheses/artificial joints: dermatitis in orthopedic surgeons � Cross-reacts with ethyl methacrylate three. Toluene-sulfonamide (tosylamide) formaldehyde resin � Used in nail polishes � Nail polish: eyelid, face, neck, finger dermatitis � � 6. Alliaceae � Genus Allium � Includes onions, garlic, and chives � Allergens: diallyldisulfide, allylpropyl disulfide, and allicin � Fresh garlic is both an allergen and a potent irritant � Causes second- and third-degree burns when applied to injured skin � Most common explanation for fingertip dermatitis in housewives and caterers three. Lichens � Allergens: usnic acid, atranorin, evernic acid, fumarprotocetraric acid � Forest workers, gardeners, woodcutters � Lichen extracts (oak moss, tree moss): dermatitis from aftershave products four. Liliaceae � Tulips, hyacinths, and asparagus � Tulip fingers � Combined allergic and irritant contact dermatitis � Allergen: tuliposide A is transformed to tulipalin A, the allergen, by means of acidic hydrolysis eight. Alstroemeriaceae household (Peruvian lily) � Tuliposide A and B are found in just about all parts of the plant � Flowers comprise more allergen than the stems; the leaves have the smallest quantity of allergen � Most frequent cause of allergic hand dermatitis in florists 9.
Cheap malegra dxt 130 mg
Proximally erectile dysfunction injection medication 130 mg malegra dxt amex, the sheaths prolong for a brief distance proximal to the extensor retinaculum erectile dysfunction questions cheap malegra dxt 130 mg with visa. Distally, the sheaths of tendons that achieve insertion into the bases of the metacarpal bones extend up to the insertion. The sheath for the extensor pollicis brevis extends to the bottom of the first metacarpal bone. The sheaths for the tendons going to the digits, and that for the extensor pollicis longus, lengthen to the level of the center of the metacarpus. Supinator crest of ulna and posterior part of triangular area in entrance of it Insertion Action Nerve Supply Deep branch of radial nerve (C7, 8) Upper one-third of lateral Supination of the arm floor of radius. Extends distal phalanx Deep department of radial nerve floor of ulna (below thumb (dorsal aspect) of thumb origin of abductor pol2. Radial side of the bottom Abduction and extension Deep department of longus of thumb (at carpometa- radial nerve floor of ulna. Helps to lengthen the wrist radial nerve (C7, 8) tensor digitorum tendon for the index finger (and is not directly inserted into the center and distal phalanges) Extensor pollicis brevis 1. Posterior floor of ra- Dorsal floor of the base Extends proximal phalanx Deep department of dius (below origin of ab- of the proximal phalanx of and metacarpal bone of radial nerve the thumb the thumb (C7, 8) ductor pollicis longus) 2. The nerve provide to muscles on the again of the forearm is through the deep department of the radial nerve. The dorsum of the hand is provided by branches of the radial, ulnar and median nerves. Joints may be classified into varied sorts depending upon their construction and on the movements permitted by them. The cranium bones are lined on the outside by a membrane called the pericranium, and on the within by one other membrane known as the endocranium (which is the outer layer of duramater). The sutures begin disappearing (by fusion of the bones) around the age of 30 years, the fusion beginning first on the endocranial surface and steadily extending to the outer surface. Sutures are of various types relying on the form of the bone ends as proven in 7. The joints between the enamel and jaws are additionally fibrous joints, the cavity within the jaw and the basis of the tooth being connected only by some fibrous tissue. The inferior ends of the tibia and fibula are directly united by fibrous tissue, which is in the type of a powerful ligament (7. In younger individuals most lengthy bones consist of a central half (corresponding to the shaft) referred to as the diaphysis, and of bony ends or epiphyses (7. Each epiphysis is united to the diaphysis by a plate of hyaline cartilage known as the epiphyseal plate. A joint could additionally be stated to exist between the epiphysis and the diaphysis by way of this plate. After full development is attained (by the age of 18 years or so) the epiphyseal plates of assorted synchondroses disappear and the epiphyses and diaphyses fuse. A synchondrosis is present between the our bodies of the sphenoid and occipital bones. The joint between the primary costal cartilage and the manubrium sterni is a synchondrosis. The two layers of hyaline cartilage are united by an intervening layer of fibrocartilage. In the case of the joints between the vertebral bodies, the plate of fibrocartilage is represented by the intervertebral discs. To facilitate this movement the articular surfaces are coated by a layer of hyaline cartilage (articular cartilage). This membrane secretes synovial fluid that has a lubricating and nutritive operate. Synovial joints may be categorised on the basis of the shapes of the articular joint surfaces, as follows: a. In a quantity of joints of the physique a convex articular floor on one bone matches into a concavity on the opposite bone (as proven in 7. When the convex surface is rounded (like a part of a sphere) and the concave surface is cup shaped the joint is claimed to be of the ball and socket variety (7. The point to observe is that the convex factor being spherical axis ab is roughly equal to cd. In some circumstances, one bone end may have two convex surfaces (or condyles) that fit two concavities on the alternative bone (7. The two convexities may be continuous, being separated only by a ridge (as in interphalangeal joints). An extreme example is the temporomandibular joint by which the 2 condyles lie in separate joint cavities (the right and left temporomandibular joints together constituting a condylar joint). In some instances, one bone end may be convex in a single path and concave in one other. In a pivot joint, one rod-like (or cylindrical) factor fits into a hoop formed partly by bone and partly by ligaments. About sutures it could be noted that on the time of delivery, the fibrous tissue of the sutural ligaments is sufficiently lax to allow over-riding of cranium bones on one another. Syndesmoses and gomphoses are usually included amongst immovable joints, however they do permit slight movement that affords resilience to these joints. In the case of the vertebral column the movements between succeeding vertebrae get added together in order that the entire motion turns into appreciable. These joints provide resilience to areas like the wrist and ankle, and improve the entire vary of motion in these areas. A saddle joint permits flexion, extension, abduction and adduction like an ellipsoid joint. The knee can be a hinge joint of the condylar selection, but due to differences in the dimension and form of the medial and lateral femoral condyles the actions of the knee are associated with some rotation. Functionally the 2 halves (medial and lateral) of the trochlea perform as two condyles. Yet another instance of a hinge joint is seen on the ankle the place side-to-side movement and rotation are prevented partly by the pulley like form of the upper floor of the talus, and partly by the presence of the medial and lateral malleoli on both aspect of the talus. From the above it could be famous that the time period hinge joint refers to a practical entity and not to a structural one. From what has been stated above it goes to be clear that ball and socket joints are multiaxial, ellipsoid and saddle joints are biaxial, and hinge joints are uniaxial. In the superior radioulnar joint the ring [formed by the radial notch of the ulna and the annular ligament (7. A compound joint is one during which greater than two bone ends are enclosed inside a single capsule. For example, within the elbow we really have three separate joints within one capsule: the humeroulnar, the humeroradial, and the superior radioulnar. A complex joint is one by which the cavity is divided fully or incompletely into two parts by an intraarticular disc of fibrocartilage. For example, the upper part of the temporomandibular joint permits ahead and backward gliding; and its lower half acts like a hinge joint. The discs of the sternoclavicular and inferior radioulnar joints act as necessary bonds of union between the bones concerned.
Order malegra dxt 130 mg otc
The prosthesis is positioned in a surgically created fistula connecting the posterior tracheal and anterior oesophageal walls erectile dysfunction treatment garlic 130 mg malegra dxt fast delivery. Oesophageal speech is produced by expelling air trapped in the upper oesophagus erectile dysfunction and testosterone injections malegra dxt 130 mg cheap otc, with a passable end in solely about one in 5 sufferers. These include the upper and lower alveolus, tooth, lips and the anterior two-thirds of the tongue. Betel nut chewing is a significant explanation for carcinoma of the oral cavity in sufferers from the Indian subcontinent. Hard palate Lips, buccoalveolar sulci and alveoli Anterior faucial pillar (posterior boundary) Inner surface of cheeks Inner two-thirds of tongue and floor of mouth. Carcinoma of the lip Carcinoma of the lip is frequent in outside staff and in regions close to the equator, presumably due to the consequences of ultraviolet gentle. Step 2 Post-wedge excision Larger tumours would require native pores and skin flaps for reconstruction. Radiotherapy in small early lesions also produces excellent outcomes, and control may be achieved using the argon laser. Any neoplastic lesion requiring less than a 3rd of the lip to be excised could be eliminated by a modified V incision and first closure. Carcinoma of the tongue the incidence of tongue most cancers is diminishing because of enhancements in dental hygiene and the fall in reputation of chewing tobacco. If allowed to develop, the lesion will finally cause tongue fixation and invade the mandible. Neoplasia of the oral cavity Pain is usually a serious function and signifies deep invasion. The former cancer tends to extend along the perineural spaces of the greater palatine nerves and will unfold into the skull. Treatment of adenoid cystic carcinoma is surgical procedure, presumably adopted by postoperative radiotherapy. After surgical resection, reconstruction of the delicate tissue usually entails a neighborhood flap for small defects or a free flap for giant defects. A selective or modified radical neck dissection is usually required for nodal metastases. Carcinoma of the buccal lining the buccal lining is a quite common website for most cancers on the Indian subcontinent, probably resulting from metaplastic change included by betel nut chewing. Carcinoma of ground of mouth Squamous carcinoma at this web site can present as an ulcer or as a white or pink patch. Carcinoma of the alveolar ridge the lower alveolar ridge is most commonly affected. The mandible is invaded by tumour either directly or via the inferior dental nerve canal. In the latter Clinical features Dysphagia and odynophagia (pain on swallowing) are frequent signs. Palpation of a lesion in the oral cavity will yield extra info (texture, dimensions, fixity, and so forth. Soft tissue surgical defects are greatest changed in order to maintain mobility in any tongue remnant and to help mastication and articulation. The majority of tumours are malignant squamous cell carcinomas, however lymphoma and minor salivary gland lesions can also occur. A full assessment of the extent of the lesion and a biopsy are needed and may entail a general anaesthetic. Management Treatment involves radiotherapy for early lesions or mixed chemotherapy and radiotherapy for more advanced cancers of the oropharynx. In the absence of neck node metastases, radiotherapy or chemoradiotherapy is used alone. If neck nodes exist, a modified neck Lymphoepithelioma of the oropharynx A variant of squamous carcinoma is the lymphoepithelioma. Immunocytochemistry shall be required in instances where the squamous cell Clinical options the tonsil is the same old web site affected and presents as a easy unilateral Neoplasia of the oropharynx a hundred and five. A tonsillectomy will be required, and the specimen examined histologically to determine the cellular immunology and the surface markers. Management Treatment includes radiotherapy for localized lymphoma, and over twothirds of sufferers will be cured. Rare salivary gland neoplasms include lymphoma, haemangioma and metastatic illness. Pleomorphic adenomas have a false capsule, so that simple enucleation is liable to leave residual tumour. This often entails resecting the parotid tissue (in which the adenoma is located) superficial to the facial nerve. In such cases a total parotidectomy with preservation of the facial nerve is performed. A margin of normal tissue ought to always be excised to make positive that all tumour projections from the main tumour mass are included in the resection. Welldifferentiated lesions behave as benign tumours, however an undifferentiated look is indicative of a high degree of malignancy with a propensity to native and systemic metastases. Painful enlargement might happen in affiliation with higher respiratory tract infections, owing to inflammation of the lymphoid tissue contained inside the tumour. Acinic cell tumour the acinic cell tumour predominantly arises within the parotid gland. Treatment is by surgical excision with preservation of the facial nerve if it is free of tumour. Thus, at meal instances, the affected person experiences pain, inflammation and sweating of the pores and skin over the parotid region. The nerve involvement might be as a outcome of the spread of most cancers by perineural lymphatics, which is a feature of adenoid cystic carcinoma. The facial nerve is sacrificed in order to embody most cancers cells that will have spread in perineural lymphatics. Facial weak spot after submandibular gland surgery is because of harm of the mandibular department of the facial nerve. Malignant salivary gland tumours are more probably to happen in the submandibular and minor salivary glands. Miscellaneous malignant salivary gland tumours Adenocarcinoma and squamous cell carcinoma are rare tumours in salivary glands. Neoplasia of the auricle the commonest tumours encountered within the auricle are squamous cell and basal cell carcinomas. Squamous cell carcinoma is treated by mastoidectomy and elimination of the parotid gland and temporomandibular joint. Neoplasia of the center ear Tumours confined purely to the center ear are rarely encountered. By the time of presentation most will have spread to the exterior meatus and so it may be troublesome to verify the first website of origin.