Kamagra oral jelly 100 mg buy with visa
The carcinoma cause-specific demise rates between the two treatment groups was considerably completely different (p = 0 erectile dysfunction niacin 100 mg kamagra oral jelly generic mastercard. Tse and colleagues80 carried out gene evaluation on microdissected paraffin embedded fixed-tissue archival samples erectile dysfunction doctor nashville kamagra oral jelly 100 mg generic free shipping. Mutational allelotyping targeting 9 genomic loci utilizing 15 polymorphic microsatellite markers situated in proximity to identified tumor suppressor genes function markers for the presence of gene deletion. They generally present with a palpable mass in the superotemporal orbit and proptosis, and ~40% complain of orbital ache. The neoplastic cells are pleomorphic, mitotically energetic, and arranged in sheets and cords. The tumor may produce mucin or form lumina, and bear sebaceous differentiation, rendering it indistinguishable from carcinoma of the sebaceous glands of the eyelid. Optimum therapy for this malignancy has not been properly outlined due to the small variety of reported cases. Exenteration adopted by radiation therapy appears to be an effective combination. One affected person within the treatment group was alive with proof of native unfold of the tumor; two patients died with metastasis. If the regional lymph nodes are concerned, radical neck dissection should be thought-about at the time of orbital surgery. Shields reported a patient who demonstrated clinical indicators and symptoms of a presumed pleomorphic adenoma which had been quiescent for greater than 60 years before evolving into malignant growth. The malignancy could additionally be focal and requires extensive sampling to determine, or may be readily apparent upon sectioning. Microscopically, tumor infiltration into adjoining soft tissues and bone may be seen. Even with complete resection, mortality remains excessive, with 50% of sufferers succumbing to the disease by 12 years. Individual cell traits include acinar, intercalated duct-like, vacuolated, clear and nonspecific glandular morphologies. As a modified minor salivary gland, the lacrimal gland accommodates acini that produce zymogen granules. On electron microscopy, attribute features of acinar cells embody cytoplasmic, electron-dense, round to oval, membrane-bound granules analogous to the zymogen granules of serous cells. Clinically, it often causes bony erosion and ache secondary to perineural invasion. It is characterized by a pure proliferation of keratinizing malignant squamous cells that are reasonably or properly differentiated. This domestically aggressive tumor originates from the ductal epithelial cells of the lacrimal gland and accounts for only 1�2% of lacrimal gland tumors. The mucus-secreting cells and cystoid spaces inside the specimen stain positively with mucicarmine and alcian blue stains, as nicely as the periodic acid-Schiff reaction. Grade 3 lesions, which have a worse prognosis, require exenteration and radiotherapy. Eviatar88 reported seven of eight sufferers with low-grade tumors surviving after extirpation, with or without radiation remedy. However, only one of eight sufferers with high-grade tumors remained tumor free at four years follow-up. Metastatic work-up for lung and mediastinal involvement is necessary for grade three tumors. Patients normally current with symptoms attribute of malignancy, together with pain and bony erosion. Histologic examination reveals variable proportions of ductal and huge, clear-staining, myoepithelial differentiated cells. Myoepthelial cells are located between the luminal epithelial cells and the basal lamina of the acini and the intercalated ducts of the lacrimal gland. This characteristic biphasic mobile arrangement of ductal cells and myoepithelial cells helps to differentiate this tumor from other more common circumstances similar to adenoid cystic carcinoma. Orbital exenteration with adjuvant radiation therapy could also be warranted in the treatment of this uncommon tumor. This malignant combined tumor consists of each carcinomatous and sarcomatous parts. This tumor should be thought of within the differential analysis of a lacrimal gland mass if sarcomatous elements are encountered on histologic examination. Mindlin A, Lambert D, Barsky D: Mixed lacrimal gland tumor arising from ectopic lacrimal gland tissue in the orbit. Bolzoni A, Pianta L, Farina D, Nicolai P: Benign myoepithelioma of the lacrimal gland: report of a case. Kiratli H, Bilgic S: An uncommon scientific course of adenoid cystic carcinoma of the lacrimal gland. Polito E, Leccisotti A: Epithelial malignancies of the lacrimal gland: survival rates after intensive and conservative remedy. Janecka I, Housepian E, Trokel S, et al: Surgical administration of malignant tumors of the lacrimal gland. Tsukuda M, Kokatsu T, Ito K, et al: Chemotherapy for recurrent adeno- and adenoid cystic carcinomas within the head and neck. Rolston R, Sasatomi E, Hunt J, et al: Distinguishing de novo second most cancers formation from tumor recurrence: mutational fingerprinting by microdissection genotyping. De Rosa G, Zeppa P, Tranfa F, Bonavolonta G: Acinic cell carcinoma arising in a lacrimal gland: first case report. Hotta K, Arisawa T, Mito H, Narita M: Primary squamous cell carcinoma of the lacrimal gland. Fenton S, Srinivasan S, Harnett A, Brown I: Squamous cell carcinoma of the lacrimal gland. There is often alteration of the higher eyelid contour, and downward and nasal displacement of the globe. In regards to the suspected etiology, the clinician ought to contemplate the axiom: "Half and half; then half again. Normal contour of the upper eyelid is deformed into an S shape with enlargement of a mass in the lacrimal gland fossa. Erythema, chemosis, tenderness on palpation, and pain with extraocular motion normally signify inflammatory disease. The pain related to perineural invasion in adenocystic carcinoma normally occurs after a mass is seen or proptosis commences. Rarely symptomatic is the diminution in lacrimal gland secretions due to any of those processes.
Kamagra oral jelly 100 mg mastercard
Plump fusiform and dendritic cells (intermediate between plump polyhedral and slender spindle cells) erectile dysfunction gene therapy kamagra oral jelly 100 mg purchase with visa, with reasonable pigmentation doctor for erectile dysfunction philippines order kamagra oral jelly 100 mg otc, a barely bigger nucleus, and occasionally a small nucleolus. Balloon cells, that are giant, amelanotic, and polyhedral with distended finely vacuolated cytoplasm. Compared with malignant melanomas, most small choroidal and ciliary body nevi have minimal results on adjacent tissues. Yanoff and Zimmerman263 instructed that almost all malignant melanomas of the choroid and ciliary body come up in preexisting nevi, as they demonstrated that seventy three of 100 consecutive malignant melanomas had nevus cells within or alongside their edges. In a single research, RodriguezSains264 reported that patients with the dysplastic nevus syndrome have an increased incidence of uveal nevi. Melanocytoma is a rare heavily pigmented lesion, which is clinically necessary as a outcome of up to now, it was incessantly misdiagnosed as malignant melanoma and was treated inappropriately by enucleation. In contrast to malignant melanoma, optic disk melanocytomas are extra widespread in closely pigmented races than in whites, though 80% of ciliary physique melanocytomas happen in whites. Macroscopically, melanocytomas are composed of plump polyhedral nevus cells, with cytoplasm distended by heavily pigmented melanosomes. Melanin bleach preparations to confirm that cell nuclei are small and spherical, without nucleoli or mitotic figures. Ciliary body and iris melanocytomas usually bear spontaneous necrosis, and this will likely trigger seeding into the anterior chamber angle and secondary open-angle melanomalytic glaucoma. In uncommon cases, malignant melanomas have arisen in uveal and optic nerve head melanocytomas. These circumstances are brought on by a failure of migration of melanocytes to their regular resting position within the surface epithelium. Oculodermal melanocytosis, affecting the eyelid pores and skin and episclera (a), with (b) diffuse choroidal pigmentation. Pathology of the Uveal Tract the pigmentary change is confined to the sclera and episclera with out involvement of the pores and skin, the term ocular melanosis is used. Clinically, this situation offers rise to slate grey or bluish look of the sclera, as opposed to the dusty brown appearance of major acquired melanosis or racial melanosis. The pigment throughout the sclera has the distinctive function of outlining the blood vessels. The diffuse involvement of the uveal tract can provide rise to iris heterochromia and a darker look to the fundus on the affected facet. Gonder and associates284 estimated the prevalence of ocular melanocytosis to be zero. In the same study, the prevalence of oculodermal melanocytosis in black patients (6915 sufferers examined) was found to be zero. The prevalence of ocular melanocytosis within the Asian population is larger, with a reported prevalence between 0. Two research have calculated ocular melanocytosis to be 30 to 35 times extra frequent in patients with uveal melanoma. Uveal malignant melanoma is uncommon in black sufferers: it occurs in 1% of African Americans301 and possibly even much less in African black persons. Congenital melanosis304�306 and uveal nevi250,307,308 are both significant risk elements within the improvement of uveal malignant melanoma, although malignant tumors occur more incessantly in ocular melanocytosis and oculodermal melanocytosis (nevus of Ota) than in nevi. Uveal malignant melanoma has been reported to have an result on successive generations of a small variety of households,245,310�312 but heredofamilial malignant melanoma is extremely rare. It seems that individual members of those households have a low absolute threat of growing tumors, although this threat is considerably larger than for people in the basic inhabitants. However, no particular genetic defects have been found in most patients with uveal malignant melanoma. Specific nonrandom chromosomal abnormalities are widespread in uveal and, particularly, ciliary body malignant melanomas. The affiliation between uveal malignant melanoma and preexisting uveal nevi, melanocytosis, and dysplastic nevus syndrome was discussed earlier. Malignant Neoplasms Posterior uveal (choroidal and ciliary body) malignant melanoma the term uveal malignant melanoma is beneficial by the World Health Organization289 and the Armed Forces Institute of Pathology to name the malignant neoplasm arising from uveal tract melanocytes. Uveal malignant melanoma (that arises in the choroid and the ciliary body) is the commonest primary intraocular malignancy in adult humans247: Most occur within the choroid (85%), and a few occur within the ciliary physique (10%) and the iris (5%)290 Overall, uveal malignant melanoma is a highly aggressive neoplasm, and about half of patients with this kind die of disseminated tumor within 10�15 years of diagnosis, though deaths from metastasis can happen even 30 years after diagnosis. Congenital uveal malignant melanoma is known but extraordinarily uncommon,294,295 and Shields and colleagues296 reported that only 1. The incidence of uveal malignant melanoma was greater in men (55%) than in ladies (45%) in 4995 patients within the Armed Forces Institute of Pathology Registry of Ophthalmic Pathology within the United States in 1994,245 and a predominance Clinical features the clinical features of uveal malignant melanoma rely upon the positioning and the stage of the tumor. Asymptomatic, found by the way on routine eye examinations; small tumors confined to the uvea, with attainable small scotoma related to degeneration of overlying retina Stage 2. Progressive blurring and lack of imaginative and prescient ensuing from retinal degeneration and detachment Stage 3. Ocular pain as a outcome of associated glaucoma (pupillary block, rubeosis, or angle invasion) or inflammation Stage four. Effects of extraocular extension, such as subconjunctival mass and proptosis Between 1936 and 1975, the Registry of Ophthalmic Pathology on the Armed Forces Institute of Pathology recorded 2627 instances of uveal malignant melanoma: 3% offered at medical stage 1, 64% at stage 2, 32% at stage 3, and 1% at stage four. This discovering means that the process of metastasis happens comparatively early in the natural historical past of the disease. Eventually, half of the patients with malignant melanoma die of disseminated disease inside 10�15 years of analysis. As the tumor enlarges, the overlying retina undergoes atrophic or cystoid degenerative adjustments, with progressively more in depth exudative retinal detachment. Large, nodular tumors could ultimately invade and destroy adjoining intraocular tissues, filling the posterior chamber. Subsequent enlargement could displace the iris and lens anteriorly, inflicting progressive narrowing of the anterior chamber angle and eventual obliteration of the anterior chamber. Scleral invasion is extra widespread within the diffuse than in more nodular tumors,244 and so they are inclined to trigger disproportionately giant orbital tumor deposits. They commonly invade the iris root and the drainage structures of the anterior chamber. Displacement of the lens, lenticular notch, and cataract formation are additionally possible penalties of ciliary body malignant melanomas. Diffuse infiltrating malignant melanoma additionally happens within the ciliary body, the place it might produce a circumferential ring development sample. Disproportionate extraocular spread is a typical consequence of this type of malignant melanoma and it has a poor ocular and systemic prognosis. Diffuse infiltrating malignant melanoma (a) is flat, with in depth subretinal extension. This tumor (b) is less than 2 mm thick and is extremely pigmented, with amelanotic areas.
100 mg kamagra oral jelly generic
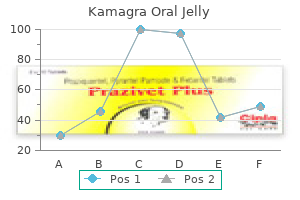
Metastasis erectile dysfunction protocol hoax cheap 100 mg kamagra oral jelly fast delivery, normally to the lung erectile dysfunction statistics canada cheap kamagra oral jelly 100 mg online, may happen 5�10 years after the diagnosis is made. Dosimetry curves for a patient with adenoid cystic carcinoma of the lacrimal gland being treated with proton beam therapy. Note the high focus of the therapy on the gland mattress and along its perineural course. At her final examination, virtually 9 years after her presentation, she has normal binocular vision. Her corrected imaginative and prescient has been decreased one line to 20/40 due to high myopic modifications. She solely suffered keratitis sicca on the affected aspect in the course of the first year following therapy. Malignant Mixed-Cell Tumors Malignant mixed-cell tumors account for less than 10% of all epithelial tumors of the lacrimal gland. These tumors most often arise within or adjoining to benign pleomorphic adenoma29 and are more regularly related to recurrent benign blended tumors displaying speedy growth. The surgical specimen of the adenoid cystic carcinoma with adjoining bone still attached. The globe is unbroken and there no sign of recurrence at the tumor website or alongside the perineural course. In any case, these patients must be monitored by each the ophthalmologist and the oncologist with examinations and scans for several years earlier than cheap assurance of cure can be assumed. The characteristic salmon-colored mass can generally be seen within the superolateral cul-de-sac, however more typically the palpable mass is fixed to the orbital rim and is rubbery. The age incidence of lymphoma of the lacrimal gland appears bimodal, with peaks in each the third decade and the sixth. Full-body scanning and bone marrow biopsies are commonplace early investigative techniques. Some oncologists argue that lymphoma is a systemic illness which will initially current in the orbit and, subsequently, prescribe systemic chemotherapy. The incontrovertible truth that half of all patients with orbital lymphoma Other Primary Malignancies Other kinds of carcinomas occurring in the lacrimal gland embrace adenocarcinoma, squamous cell carcinoma and mucoepidermoid carcinoma. Interestingly, this last type is sort of rare within the lacrimal gland but happen much more regularly in the salivary glands. Sinus tumors hardly ever invade the gland due to the distance from even the most lateral portion of the frontal sinus. However, basal cell carcinoma at the lateral canthus, squamous cell carcinoma from the conjunctiva, or even sebaceous cell carcinoma from the lid might present with the bulk of its mass in the lacrimal fossa. Inflammatory and neoplastic traits are useful in directing the plan of action. Suspicion of pleomorphic adenoma will appropriately information clinicians in their surgical management. Bilateral painless enlargement of the lacrimal glands led to this referral for remedy of mechanical ptosis. Tumors of the Lacrimal Gland and Sac to the nasopharynx, in the presence of noticed epiphora is one other suspicious indicator. Spontaneous bleeding31,32 from the punctum must at all times be regarded with a high index of suspicion. Bilateral exposures with posteroanterior and lateral views allow comparisons to be made. A late movie (30 min) must be taken to help assess the emptying time of the two sides. A low-viscosity contrast medium (Ethiodol or Pantopaque) is superior to aqueous or highly viscous materials33�37 for this software. Filling defects may be because of intrinsic masses such as dacryoliths38 or neoplasia. A tumor throughout the sac changes the conventional concave look of the wall to a scalloped border. Extrinsic plenty compress the sac wall and convert the traditional concave define to one with a convex element. Anteroposterior view of a dacryocystogram demonstrates a transparent area throughout the sac. Plaster casts with lacrimal systems (after Whitnall) show the variation in diverticula. Anterior extension of the ethmoidal sinus can lengthen anteriorly to the lacrimal sac. Additionally, the sac accommodates scattered goblet cells, mucus secretors, and serous glands. The exact incidence of diverticula is uncertain, however their presence has been repeatedly noted throughout anatomic dissections and surgical procedure. Diverticulitis of the lacrimal sac has been observed during the latter a half of being pregnant. The most typical cyst-like lesion is the mucocele,31 associated with concurrent nasolacrimal duct obstruction. When the lumen of the sac becomes infected and purulent secretions fill the sac, the mass is referred to as a pyocele. An ethmoidal mucocele may also extend anteriorly without lacrimal sac involvement. When this does occur, the cystic structure can usually be recognized superior to the medial canthal tendon. Another external cystic lesion that will impinge on the lacrimal sac is a dermoid cyst. Rare reported causes of cystic lots inside the lacrimal sac are trauma and congenital malformation. This latter cause is exclusive in that the cyst throughout the sac has a complete and separate wall. After persistent software of topical epinephrine,45 melanin-laden casts have formed throughout the sac. Demonstration of an ethmoidal mucocele obstructing the flow from the lacrimal sac to its duct. Sarcoidosis50,fifty one has been demonstrated throughout the lacrimal sac in patients with respiratory manifestations of this noncaseating granulomatous illness. Before profitable chemotherapy for this disease, few patients lived lengthy sufficient to present with epiphora. Once once more, routine biopsy of the lacrimal sac may be the preliminary diagnostic event for these sufferers.
Kamagra oral jelly 100 mg buy cheap
The rarity of mitotic figures and the abundant mucin secretion are proof of the excessive degree of cellular differentiation erectile dysfunction caused by high cholesterol kamagra oral jelly 100 mg buy online. An eccrine origin is borne out by the work of Headington erectile dysfunction under 35 kamagra oral jelly 100 mg generic on-line,106 who notes a robust reaction for oxidative enzymes, succinic dehydrogenase, lactic dehydrogenase, and isocitric dehydrogenase. Adenosine triphosphatase, acid phosphatase, and nonspecific esterase are weakly positive. With electron microscopy, the dark cells seen on hematoxylin and eosin stain contain skinny filaments, membrane-bound dense granules, and numerous secretory vacuoles that coalesce to kind massive subplasmalemmal vacuoles. The gentle cells have a paucity of organelles and comprise small whorls of cytoplasmic filaments and tough endoplasmic reticulum. The histologic differential prognosis contains metastatic mucinous carcinoma arising from the gastrointestinal tract, breast, or ovary. The mucin histochemical traits of metastatic lesions are, nevertheless, distinct from most main mucinous lid lesions. When stained with alcian blue, this mucin is hyaluronidase-sensitive and sialidase-resistant (the reverse of mucinous adenocarcinoma). Finally, mucinous adenocarcinomas with strong patterns might resemble eccrine poromas or, much less probably, spiradenoma. Mucinous adenocarcinoma of the lid could infiltrate the local tissues and lengthen into the orbit. Cohen and colleagues108 reported the case of a 62-year-old lady who introduced with a recurrent medial canthal lesion. The skin overlying the tumor was freely movable, however the mass was fixed to underlying bone. At surgical procedure, the mucinous adenocarcinoma hugged the medial wall, extending half method to the orbital apex. Khalil and associates109 described a 70-year-old man whose tumor invaded the orbit, optic nerve, sclera, and ethmoidal sinus over a 25-year interval. Long-term follow-up information means that mucinous adenocarcinoma has a greater prognosis than do other sweat gland carcinomas. Eight patients had a quantity of native recurrences, and just one patient skilled submandibular node metastases. El-Domeiri and colleagues116 reported 63 patients who had mucinous adenocarcinoma affecting varied elements of the body and who had been monitored for five years or extra. Regional lymph node metastases developed in 43% of patients, and 38% skilled widespread metastatic disease. Optimal administration consists of extensive en bloc resection of the tumor with frozen section management. The tumor progresses slowly, can involve the other ipsilateral lid, recurs after inadequate excision, and occasionally results in regional and distant metastases. Histologically, the well-differentiated ductal carcinoma options quite a few signet-ring cells and has been categorized as signet-ring adenocarcinoma. At excessive power, some of the cells have a wavy look with comma-shaped nuclei suggestive of a neurofibroma. The mobile infiltrate consists in a part of cells rising diffusely in small cords or in single file in a fibrotic stroma. In distinction, the poorly differentiated ductal carcinoma options has been categorised as histiocytoid eccrine ductal carcinoma. Granular cell myoblastoma, neurilemoma, an inflammatory infiltrate composed of histiocytes, and histiocytoid mammary carcinoma metastatic to the eyelid have been mistakenly confused for major ductal adenocarcinoma. A clinical analysis must then be undertaken to exclude a primary neoplasm elsewhere. The vertical palpebral fissure is narrowed owing to upper eyelid involvement as nicely. Ultrastructural research reveal intracytoplasmic lumina with villi, ample smooth and tough endoplasmic reticulum, lipid droplets, and filamentous granular cytoplasmic inclusions. Rosen has proposed an eccrine origin, based on the ultrastructural findings of light and dark cells. Antiestrogen remedy has additionally been tried as an adjunct as a end result of the tumor might specific estrogen and progesterone receptors. One of the circumstances was initially estrogen receptor constructive, was handled with Tamoxifen, however developed a recurrence and upon repeat biopsy was estrogen receptor unfavorable. Locally aggressive, sclerosing sweat duct carcinoma has a clear-cut predilection for the higher lip, nasolabial area, and periorbita. Several authors imagine it represents another variant of a ductal eccrine adenocarcinoma. In two patients, the tumor recurred after surgical excision, however no documented metastases occurred. Cooper and coworkers125 reviewed histologic sections of ~2000 carcinomas of every kind involving the lip, nose, and periorbital area from the University of Virginia Medical Center between 1950 and 1980. These five sufferers ranged from 20 to sixty four years of age; three were men and two were ladies. Clinically, the lesions were either ill-defined indurations, firmto-hard plaques, discrete nodules, or cyst-like growths with a easy or crusted epidermal surface. A sixth patient, a 51-year-old girl, presented with tumor infiltrating the higher lip, nose, and cheek. At the final reported follow-up, 4 years after initial remedy, she was alive and had tumor infiltrating the orbit however without metastases. Histologically, these tumors are characterised by strong strands of epithelial cells with scant eosinophilic cytoplasm embedded in a sclerotic stroma. Based on the differentiation toward sweat ducts and the accompanying plentiful sclerotic stroma, some authors choose the term sclerosing sweat duct carcinoma instead of microcystic adnexal carcinoma. Histochemistry studies reveal that some tumor nests contain small amounts of collagen. Carcinoembryonic antigen has been detected around the ductal portion of the carcinoma however is absent round keratocytes. Additional cases of sclerosing sweat duct carcinoma affecting the eyelids have been reported. Computed tomography disclosed a delicate tissue mass within the inferomedial orbit extending from the orbital rim to the apex. The patients all shared in common a protracted scientific course from stromal sclerosis, tumor infiltrating the orbit along perineural planes, and the absence of lymph node metastases. Bier-Lansing and coworkers131 reported, to our knowledge, the one case of a regional lymph node metastasis. The former possess round or elongated, deeply basophilic nuclei, and scant cytoplasm. In early lesions, the basophilic cells undergo appreciable mitotic exercise, which is a normal finding in keeping with an origin from the primordial epithelium of the hair matrix or bulb. As the tumor matures, the basaloid matrical cells rework into centrally located shadow or ghost cells. These nuclei are finally misplaced, resulting in sheets of intensely eosinophilic, keratinous material.
Diseases
- Fibrous dysplasia of bone
- Lung agenesis heart defect thumb anomalies
- Childhood disintegrative disorder
- Kozlowski Brown Hardwick syndrome
- Pancreatic islet cell tumors
- Dyserythropoietic anemia, congenital type 3
- Hypertensive hyperkalemia, familial
- Adrenal cancer
- Alopecia congenita keratosis palmoplantaris
- Mental retardation epilepsy
100 mg kamagra oral jelly order visa
In benign fibrous histiocytoma erectile dysfunction caused by zoloft kamagra oral jelly 100 mg order otc, immunohistochemical research are generally unrewarding; the immunohistochemical stain for the intermediate filament vimentin is almost all the time constructive erectile dysfunction code red 7 kamagra oral jelly 100 mg discount visa, and the S100 protein staining might be negative. Electron microscopy reveals that most of the tumor cells show features of the fibroblast, specifically, rough-surfaced endoplasmic reticulum, scattered mitochondria, and the absence of extracellular basement membrane production areas. Despite its size, the lesion remains well circumscribed and partially surrounded by a pseudocapsule. The white look on the minimize floor is the outcome of deposition of collagen by the fibroblasts within the tumor. Electron microscopy of tumors with a pleomorphic malignant fibrous histiocytoma sample demonstrates ultrastuctural options of the precise lineage of cells, or might show comparatively undifferentiated cells. The benign lesions had been circumscribed, had small nucleoli inside regular nuclei, and no mitotic figures. Such lesions are able to recurrence if incompletely excised, which happened in 31% of the instances. However, the chance of malignant transformation on recurrence is small, and not considered one of the sufferers on this class died. The tumors were extra cellular, the nuclei were considerably more hyperchromatic and crowded collectively, the nucleoli were extra outstanding, and mitotic activity, which generally was not pronounced, was within the vicinity of one mitotic figure per high-power microscopic field. The domestically aggressive lesions underwent a 57% recurrence price, and the malignant lesions exhibited a 64% recurrence fee, with six of 14 patients dying directly on account of their malignancies. Widespread metastases can eventuate from four to 22 years after the primary orbital recurrence. By distinction, the domestically aggressive lesions had a 92% survival price at 10 years, whereas patients with malignancy had only a 23% survival price at 10 years. As already famous, malignant orbital fibrous histiocytomas can also arise after radiotherapy for retinoblastoma or an earlier orbital rhabdomyosarcoma. It is worth making a few comments concerning the highly distinctive appearance of fibrous histiocytoma that arises at the corneoscleral limbus. These benign lesions36 are normally acquired slowly in maturity and have a yellow appearance. Both the cornea and contiguous sclera could additionally be thickened, and the yellow appearance is more readily discernible in the corneal element, which is vascularized. Many clinicians are tempted to diagnose a dermoid or a dermolipoma, but these are always congenital lesions. Histopathologically, the benign lesions show a storiform pattern with a variable admixture of mono- and multinucleated lipidized histiocytes. Far extra ominous are the epibulbar and corneoscleral malignant fibrous histiocytomas, which may be deadly. In these lesions, immunohistochemical methods for the identification of an antimacrophage factor and electron microscopic demonstration of lysosomes are useful. Wide local excision coupled with cryotherapy to the epibulbar surface might be tried on the time of first excision, however on recurrence, severe consideration should be given to radical surgery. A malignant epibulbar fibrous histiocytoma should be distinguished from a spindle-cell squamous carcinoma,39 a spindle-cell (sometimes desmoplastic) melanoma,forty and leiomyosarcoma. The immunohistochemical staining characteristics of these tumors are summarized in Table 242. For a well-circumscribed benign fibrous histiocytoma, local excision must be sufficient remedy. Obviously, extra beneficiant margins have to be taken if the lesion has options of a regionally infiltrating and aggressive fibrous histiocytoma. For each the histologically benign and domestically aggressive forms, if a considerable amount of tumor was left behind on the time of an preliminary diagnostic orbitotomy, plans ought to be made to return immediately to try to excise the whole lesion if potential, taking precautions to protect the extraocular muscles and the nerves in the orbit, together with the optic nerve. Once a symptomatic recurrence develops, throughout which there may be evidence of elevated cellularity, plump and extra pleomorphic nuclei, and increased mitotic figures, definitive ablative surgery in all probability ought to be carried out (including attainable exenteration) to prevent unfold into a surrounding compartment or widespread metastases. For lesions which are found to be unequivocally malignant on the time of first surgical procedure, it appears that exenteration must be performed immediately to present the patient with one of the best chance for survival, except there are highly effective reasons to try one other native excision, such because the patient having only one useful eye. Furthermore, in areas of necrosis, one must be careful to not misread infiltrating bloodborne histiocytic parts as indigenous to the tumor itself. Fibrous histiocytomas must even be distinguished from major mengiomas of the optic nerve sheath, the overwhelming majority of that are transitional or meningothelial. Ultrastructurally, meningiomas show proof of intercellular imbrications of cell processes, desmosome formation, and myriad cytoplasmic filaments which have been established to be vimentin. Fibrous histiocytoma also incorporates vimentin cytoplasmic filaments, however in much less copious quantities in comparison with meningioma. Furthermore, many meningiomas show cell-surface epithelial membrane antigen positivity. Approximately one-third of orbital fibrous histiocytomas may show fields indistinguishable from those in a cellular variant of the solitary fibrous tumor, formally known as hemangiopericytoma. Some of the cells might often present proof of myofilamentary cytoplasmic differentiation. In present diagnostic pathology, a lot of what had beforehand been known as fibrous histiocytoma is now being read as solitary fibrous tumor. Fibrous histiocytoma may have conspicuous areas of myxoid stroma, in view of the fact that the fibroblast and its congeners are capable of elaborating mucopolysaccharides. In such lesions, one makes an attempt to find fields which would possibly be composed of extra compact cells in a spiral nebular or storiform sample. Neurofibroma could additionally be almost fully myxoid in nature, by which case one makes an attempt to find wavy bundles and cells with comma-shaped nuclei. Solitary fibrous tumor and liposarcoma could additionally be very myxoid; in the former one must discover compact, ovoid, reticulinensheathed cells endowed with a prominent vascularity away from the myxoid areas, whereas in the latter there ought to be a plexiform capillary sample and one searches for univacuolar lipoblasts. There are different features useful for distinguishing fibrous histiocytoma from simulating grownup spindle cell tumors, significantly peripheral nerve sheath and clean muscle tumors. The schwannoma reveals extra delicate eosinophilic cytoplasm due to the interlacing of myriad sinuous cytoplasmic processes. Electron microscopy reveals electron-lucent cytoplasm in both benign and malignant schwannomas, myriad interdigitating cellular processes, and focal to steady basement membrane formation. In fibrous histiocytoma, the tumor cells are inclined to create the spiral nebular or storiform sample, whereas in pure, basic fibrosarcomatous lesions, there are extra sleek longitudinal fascicles that interdigitate laterally in a herringbone pattern. Lesions prior to now that had been recognized as orbital fibrosarcoma in all likelihood would at present be positioned among the many fibrous histiocytomas, either regionally aggressive or malignant. Identification of round or polygonal histiocytic elements with or with out demonstrable cytoplasmic lipid points toward a fibrous histiocytoma, but these cells is probably not conspicuous in many proliferations. Histiocytic markers are usually adverse in benign fibrous histiocytomas, similar to lysozyme, common leukocytic antigen, and a1-antichymotrypsin. Some malignant fibrous histiocytomas have been variably reported to be constructive for these features, however many sarcomas, including malignant fibrous 3172 Mesenchymal, Fibroosseous, and Cartilaginous Orbital Tumors can be cavitary formation also that includes xanthoma cells.
Generic 100 mg kamagra oral jelly amex
The small nuclei are widely spaced secondary to the relatively wealthy eosinophilic cytoplasm erectile dysfunction age young kamagra oral jelly 100 mg fast delivery. Many of the cells have ample cytoplasm with perinuclear halos because of impotence beta blockers 100 mg kamagra oral jelly purchase amex the plentiful immunoglobulin-producing Golgi bodies in these cells. Therefore, all patients with ocular adnexal lymphoid lesions ought to have a systemic evaluation. The general incidence of systemic disease associated with ocular adnexal lymphoid proliferations is ~30�35% (Table 237. Orbital gentle tissue lesions (including the lacrimal gland) and conjunctival lesions are associated with systemic disease in one-fifth to one-third of instances, respectively. Alternatively, lesions localized to the preseptal portion of the eyelids solely (not an anterior extension of a deeper orbital process) are related to systemic lymphoma in about two-thirds of circumstances (Table 237. It is necessary to keep in mind that this last grouping of instances restricted to the eyelids is essentially the most rare clinical presentation, composing ~5�10% of circumstances. This discovering of a differential incidence of systemic disease, related most notably with instances restricted to the preseptal portion of the eyelid, underscores the clinical significance of creating the locus of the lymphoid proliferation via the scientific examination and adjunctive imaging through the preliminary assessment of sufferers with orbital and adnexal lymphoid proliferations. Bilateral orbital lymphoid lesions characterize an fascinating subset of ocular adnexal lymphoma. The incidence of affiliation with systemic illness has been reported to be 35%, approximating the general affiliation with systemic disease seen amongst all new sufferers presenting with orbital and adnexal lymphoid tumors. However, others have reported that bilaterality does have a major affiliation with lymphoma associated dying. Over the course of follow-up, it might be anticipated that ~20�25% of sufferers not known previously to have systemic lymphoma could have proof of disseminated disease inside 5 years. Because of the utility of medical staging, 3056 Orbital and Ocular Adnexal Lymphoid Tumors systemic evaluations of sufferers with orbital lymphoid lesions are greatest carried out by scientific oncologists with an curiosity in lymphomas. These physicians can provoke a search on orbital presentation for occult systemic illness. A bone scan, particularly if bone pain is present on presentation, and a liver�spleen scan may be helpful. These sufferers should be adopted every 6 months for at least the first yr, and as a lot as 5 years, for the reason that majority of relapses occur within this era. The diffuse infiltrating nature of orbital lesions makes their whole excision difficult and risky. Additionally, their excellent response to local lowdose irradiation obviates the need for attempted excision. In rare cases in which the lesion is extra posterior in the orbit, a lateral orbitotomy with bone removal may be essential to obtain entry and a representative biopsy. Alternatively, fineneedle biopsy coupled with particular cell surface marker research of the cytologic sample can present sufficient diagnostic material and keep away from the necessity for incisional surgical procedure. If the lesion is situated primarily within the lacrimal gland, careful preoperative assessment focusing on the beforehand addressed radiologic and scientific findings seen with lymphoid tumors is essential to set up a presumptive analysis. Conjunctival lesions are usually diffuse, and an sufficient biopsy ought to provide sufficient diagnostic tissue. However, in chosen instances, a localized conjunctival lesion may be excised simply without significantly sacrificing the conjunctival floor. In these cases, an entire excision coupled with close postoperative follow-up may stop the necessity for orbital irradiation. In cases of bilateral lymphoid tumors, only one aspect must be biopsied as a outcome of equivalent histologic features and immunophenotype are usually found bilaterally in these cases. If attainable, extra specimens should be prepared as frozen sections48,49 or cell suspensions to allow immunophenotypic or genetic analysis. Although more knowledge are made available with adjunctive immunologic analysis, a careful histologic evaluation of lymphoid specimens is economically preferable because the histopathologic findings seem to be just pretty much as good by method of predicting systemic disease. This can normally be obtained transconjunctivally in lesions which may be clinically and radiographically suggestive of a lymphoid process. The regular orbital fat (left) is seen juxtapositioned to an orbital lymphoid infiltrate (right). Gross fresh appearance of a lacrimal gland tumor demonstrates the fish-flesh character of the lymphoid proliferation. Furthermore, therapy should be delivered to the whole orbit in order to forestall recurrence in uninvolved areas. When radiation treatment is given in these low doses in a fractionated trend, problems, together with dry eye and lenticular changes, are sometimes minimal. These lesions are effectively handled with either liquid nitrogen or a double freezethaw technique utilizing a cryoprobe. During orbital irradiation, the globe and lens are protected by a metallic protect mounted on a suction contact lens. Ocular adnexal lymphoma, even when localized, should be seen as a low-grade indolent systemic disease. The effects of systemic treatment on the orbital or lid lesion should be assessed earlier than instituting orbital irradiation. If large orbital involvement threatening vision in association with systemic lymphoma is discovered on presentation, systemic chemotherapy and localized orbital irradiation could also be instituted concurrently. It is essential to bear in mind that chemotherapy potentiates the cytotoxic effect of irradiation. Therefore, this small subset patient inhabitants needs to be particularly carefully followed for ocular radiation sequelae. If a affected person is found to have systemic lymphoma, the outlook remains to be favorable as a end result of many of the lymphomas are comparatively indolent and should encompass fewer malignant cell varieties. Systemic steroids are useful in treating inflammatory pseudotumors; but when used in the presence of orbital lymphoid lesions, they invariably end in a temporary discount of the mass, adopted by a scientific rebound on cessation of the steroid. Current advances in numerous forms of immunotherapy continue to present promise within the remedy of orbital lymphoma. The disruption of the secretory acini (center), termed a lymphoepithelial lesion, is more commonly related to monoclonal proliferations. Since the affected person was discovered to have systemic disease and nonvisionthreatening orbital disease, he was handled solely with systemic chemotherapy. Malis N, Mackman G, Holds J, et al: Simultaneous and bilateral conjunctival and orbital lymphoma presenting as a conjunctival lesion. Long time period follow-up results of observation or radiation for conjunctival malignant lymphoma. Periocular mucosa-associated lymphoid/low grade lymphomas: treatment with antibiotics. This monoclonal immunoglobulin, which is commonly referred to because the M protein or myeloma protein, includes one class of heavy chains (g, a, m, d, or e) that characterize one of the 5 major immunoglobulins (IgG, IgA, IgM, IgD, or IgE) or one of many light chains (k or l). Bone pain, fatigue, and normocytic�normochromic anemia are the commonest presenting signs and indicators. Some proof of renal insufficiency attributable to Bence Jones protein obstructing the distal and accumulating tubules is present in roughly half of patients.
Buy kamagra oral jelly 100 mg with amex
Hypopigmentation of the eyelashes is more frequently encountered than hyperpigmentation erectile dysfunction at age 28 generic kamagra oral jelly 100 mg with amex. Hyperpigmentation was reported after using topical Latanoprost erectile dysfunction remedies best 100 mg kamagra oral jelly, Bimatoprost and Travapost. Clinically, this is reflected in localized depigmentation of hairs and a resultant patch of white hairs. Numerous causes of acquired poliosis are known, together with vitiligo, localized irradiation, severe dermatitis, tuberous sclerosis, neurofibromatosis, and the uveitis syndrome of Vogt, Koyanagi�Harada, and sympathetic ophthalmia. It is usually inherited as an autosomal dominant trait, caused by missense or frameshift mutation in the c-kit protooncogene on chromosome 4. Without its perform, the migration of melanoblasts from the neural crest to the dermis is arrested in sure areas throughout embryonic improvement. The situation is usually of no medical significance and can be treated by camouflage with hair dyes or dermablend or with autologous cultured epithelial grafts. This syndrome is transmitted in an autosomal dominant sample with variable penetrance of its associated anomalies. Among the related ophthalmic abnormalities are synophrys and iris heterochromia. The hairs, including the cilia, emerge at indirect angles and are fragile, quick, and sparse. Baccard M, Morel P: Excessive growth of eyelashes in patients with acquired immunodeficiency syndrome. Howaizi M: Pegylated interferon-induced eyelid and eyebrow trichomegaly throughout continual hepatitis C. Barrera A: using micrografts and minigrafts in aesthetic reconstruction of the face and scalp. Kasai K, Ogawa Y: Partial eyebrow reconstruction using subcutaneous pedicle flaps to protect the pure hair course. Webster R, Fanous N, Smith R: Blepharoplasty: when to combine it with forehead, temple or coronal raise. Hayasaka S, Noda S, Setogawa T: Epiblepharon with inverted eyelashes in Japanese children. Wolfley D: Excision of individual follicles for management of congenital distichiasis and localized trichiasis. Kumagai N, Uchikoshi T: Treatment of extensive hypomelanosis with autologous cultured epithelium. The eyelid spasms can be so severe and extended that the patient is rendered functionally blind. Even when not blinding, the disfigurement and visible impairment associated with blepharospasm are associated with diminished high quality of life. Typically, sufferers describe an preliminary period of awareness of increased blink fee. Blepharospasm is often exacerbated by stress, fatigue, brilliant lights, watching television, driving, and social interactions. A careful medication history will elucidate prior neuroleptic use that would cause tardive dyskinesia, which can be confused with blepharospasm. A household history of dystonia or postural tremor may increase the danger of blepharospasm. Blepharospasm symptoms have been reported in association with a number of focal central nervous system lesions, including decrease pontine mass,5 thalamic infarct,6 putaminal hemorrhage,7 and frontal cortical infarct. Findings on postmortem neuropathologic examination of patients who had blepharospasm alone or as a half of Meige syndrome range from no abnormality9 to neuronal cell loss, degeneration, and gliosis in varied elements of the midbrain, mind stem, and cerebellum. When the disease is obvious, the examiner will observe elevated blink rate and bilateral eyelid spasms. Ancillary Tests Magnetic resonance imaging or computed tomography scanning is pointless until different neurologic abnormalities are suspected. Similarly, different supportive laboratory, electrophysiologic, and radiologic checks are not often helpful for diagnosing essential blepharospasm or different idiopathic cranial dystonias. Treatment is directed at controlling the manifestations of the disease somewhat than curing the disorder. Oral drugs, surgical excision of involved muscles (myectomy), and surgical avulsion of the facial nerve (neurectomy) are other potential remedy options. Additionally, many patients profit from supportive measures, similar to ocular lubrication and use of tinted lenses. More than six antigenically distinct types of neurotoxins are produced by Clostridium botulinum, a spore-producing anaerobic bacillus. The toxin impact wanes as the neuromuscular junction recovers and sprouts new nerve terminals. The toxin is supplied as a lyophilized powder that should be reconstituted with sterile saline prior to injection. Due to its large size, the protein is subject to shearing if dealt with too vigorously. It is therefore essential to carefully introduce the saline into the treatment vial, directing the fluid slowly down the aspect of the vial to avoid instantly impacting the lyophilized protein. The upper eyelid injections ought to spare the central lid to minimize the chance of ptosis. Many clinicians also avoid the medial and central lower eyelid to prevent paralytic ectropion and paresis of the inferior indirect muscle. Delivery of the only decrease lid injection in an inferomedial path may maximize treatment response whereas minimizing complications. The eyelid injections must be placed near the lid margin to present longest period of effect. Several days are required for the toxin to take impact, and the medical response usually lasts 10�12 weeks. The clinician should goal to use the lowest effective dose of toxin and the least complete variety of lifetime doses. If injection with toxin A fails, use of toxin B could be thought of, as can including an oral agent or proceeding to one of the surgical options described below. Lagophthalmos causing exposure keratopathy (a) and central corneal thinning (b) 4 days after injection of botulinum toxin. Comprehensive evaluations of its history from the late eighteenth century through the appearance of intraoperative nerve stimulation may be found elsewhere. Although some practitioners46,47 report success with the operation and promote its use, there are several disadvantages to neurectomy. Second, undesirable paralysis (facial droop, mouth droop) can result even with cautious branch choice. However, botulinum toxin injections can be used to treat spasm recurrence and may provide longer-lasting paralysis after facial nerve avulsion. Because of its recognized myotoxicity, doxorubicin has been the subject of such investigation. The use of deep mind stimulation of the globus pallidus has been described for small numbers of Meige syndrome patients, with fairly dramatic, sustained spasm relief.
Buy discount kamagra oral jelly 100 mg on line
A skin-muscle (myocutaneous) flap refers to inclusion of subjacent muscle in the pores and skin flap tissue transfer depression and erectile dysfunction causes discount kamagra oral jelly 100 mg free shipping. Because of the generous vascular supply of the eyelids erectile dysfunction treatment washington dc generic 100 mg kamagra oral jelly, tissue defects as a lot as 10 cm2 could also be repaired with native flap techniques. A round defect involving the anterior lamella of the upper or lower eyelid may be converted into a sq. defect. Extensive undermining within the preseptal plane permits sufficient mobilization of skin and orbicularis muscle and recruits skin from the forgiving lateral periorbital area. After a V-shaped incision is made, the pores and skin on each side of the V is superior with the defect closed as a Y. It can be utilized to lessen the gap between the medial canthi in epicanthus or in serial style to launch skin contracture. The donor website is typically repaired with broad undermining and direct, layered closure. Tension could be released by making a short back reduce from the pivot point along the base of the flap or by making a small incision in the middle of the flap perpendicular to the line of tension. These thick flaps provide a great blood provide from each the subdermal plexus and the supratrochlear vessels. An incision is made from the superior aspect of the defect toward the middle of the glabella. The flap is rotated into the defect and anchored to the medial canthal tendon and associated deep tissues to preserve the conventional canthal concavity and to prevent webbing. To assist prevent drawing the eyebrows together, the redundant triangular tip of the flap may be excised and positioned as a graft between the eyebrows. Each flap will be about twice the diameter of the round defect and the flap ideas typically require trimming to round the distal ends. The M-plasty is another modified ellipse used to cut back the quantity of regular skin removed and to produce a shorter scar. The M-tips are closed with a half-buried horizontal mattress suture and the rest of the ellipse is closed in commonplace trend. Medially primarily based upper eyelid myocutaneous flaps can also be designed as interpolation flaps with pores and skin and muscle from a traditional upper blepharoplasty dissection transposed on a medial orbicularis oculi pedicle through a subcutaneous tunnel into the medial canthal region. The double transposition flap consists of two lobes separated by an angle and sharing a pedicle, with the smaller second flap filling the donor defect and the bigger lobe filling the primary defect. Note pores and skin marking of temporal branch of cranial seventh nerve which generally passes 1. Small area of redundancy marked out at base of flap for full-thickness pores and skin grafting (care taken not to intrude with contralateral vascular pedicle). A line is marked from the center of the 120� angles equal in length to the edges of the defect and bisecting the angle. Another line is drawn in both instructions parallel to the rhombic-shaped defect and equal in size to any facet. Because all sides are meant to appose each other after transfer they want to all be similar in length. Alternatively, uninvolved tissue adjacent to a spherical or ovoid defect could be preserved and a smaller, quasitriangular flap could be developed. As closure of the donor web site leads to a pressure vector parallel to the unincised flap base, the base of the flap is oriented parallel to the eyelid margins. The initial facet of the flap extends out radially from the defect and the second facet is drawn again towards the defect at a 60� angle. Flap closure in younger sufferers without a lot pores and skin laxity might produce dogears, which generally flatten after a quantity of months or may be excised in standard style. This flap may be 30��120� from the first flap and is normally one-half its width. After undermining and rotation of every of the flaps, the wound is closed in layers with deep absorbable sutures (Table 252. The scar, which comprises the central member, can be excised in elliptical trend. After transposition of the flaps, the central member of the resultant Z shall be at proper angles to the original central member (scar). Z-plasties with dissimilar-sized flaps can be used to handle lateral canthal dystopia. Functional and aesthetic eyelid concerns should be thought-about when addressing defects in these contiguous areas. Small- and medium-sized nonmarginal defects may be repaired by direct approximation, full-thickness skin grafting, advancement flaps, or rotational flaps as described elsewhere in this chapter. Large facial defects ensuing from Mohs micrographic surgical procedure or extensive excision of a cutaneous melanoma require a combination of reconstructive choices to reduce the aesthetic costs resulting from using large free skin grafts and extensive rotational flaps. Harris et al102,103 have outlined lots of the necessary principles that information our method to these challenging oculofacial instances. These embody extensive undermining of the tissues adjacent to the facial defect, direct wound approximation where possible, and the utilization of development flaps with deep, anchored fixation. For defects in the lateral side of the eyelid�cheek complicated, a medial-based advancement flap permits extra tissue recruitment. Nasal and temporal incision size and the quantity of flap dissection are determined by the surgeon following an intraoperative evaluation of tissue elasticity. Skin-flap mobilization is carried out by dissection above the orbicularis muscle within the decrease eyelid and inside the subcutaneous fat of the midface. In instances the place wound proximity and lower eyelid laxity increase the danger of postoperative lower eyelid malposition, a lateral tarsal strip procedure is carried out. Useful anchor factors embody the medial canthal tendon, maxillary periosteum inferior to the tendon, and the periosteum overlying the inferior or lateral orbital rim or malar eminence. We sometimes use a 4�0 polyglactin suture passed in buried style through the subcutaneous tissue of the flap and acceptable anchor level. Subdermal, buried 4�0 or 5�0 polyglactin sutures can then be used to approximate the wound edges beneath minimal tension. Skin closure is completed with 6�0 nylon or polypropylene sutures in interrupted, vertical mattress, or operating fashion as indicated. Reconstruction of eyebrow defects should embody extensive undermining and direct closure with 3�0 or 4�0 polyglactin or polyglycolic acid sutures passed in buried, interrupted trend to obtain secure subdermal assist. The skin is closed with 6�0 nylon or polypropylene sutures in vertical mattress trend to obtain good wound eversion. Plucking of medial brow hairs may be necessary because the heads of each forehead are superior medially. Large defects in the forehead and temple areas might require a combination of strategies for reconstruction. Care must be exercised throughout broad undermining within the temple area and lateral forehead to keep away from injury to peripheral branches of the cranial seventh nerve. Direct horizontal tissue development with deep closure should be attempted to close as a lot of the forehead wound as potential taking care to align any stress-free incisions within current forehead furrows. Small rotational flaps and/or full-thickness pores and skin grafts could also be necessary to close any residual defects. Secondary brow elevation, blepharoplasty, and scar revision surgical procedure could be performed as wanted in advanced cases.