Isoptin 120 mg buy low price
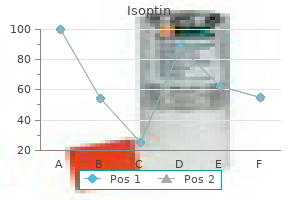
Combination formulations of acetaminophen arterial blood gas test isoptin 40 mg discount line, butalbital (a barbiturate) blood pressure 7949 240 mg isoptin order with amex, and caffeine are additionally efficient in aborting migraine headaches. Isometheptene, an agent that acts as a sympathomimetic, can terminate migraine complications. It is out there in a preparation that additionally accommodates acetaminophen and a mild sedative drug. Opioid analgesics can relieve the ache of migraine headaches, but their use should be reserved for patients in whom other agents are contraindicated or ineffective. Tramadol has been significantly useful in chronic ache syndromes (see Chapter 23) and is certainly one of the most generally used opioid drugs for the treatment of migraine. Butorphanol acts as an agonist at opioid receptors and a blended agonist-antagonist at � opioid receptors. The antipsychotic agent prochlorperazine is efficient in aborting unremitting migraine headache when given intravenously. Acupuncture and physiotherapy may be useful, however their efficacy has not been established in controlled, medical trials. The efficacy of those brokers varies from affected person to affected person, nevertheless, so finding a drug that works well is largely a matter of trial and error. The aim of prophylactic drug use is to reduce the frequency of migraine attacks by at least 50%, and the factors for evaluating the efficacy of specific medicine must be clearly established and understood by the physician and patient. It usually takes three to 4 weeks of therapy earlier than the benefit of a given drug is noticed, so authorities advocate a trial of four to 6 weeks before switching to one other drug. The best drug to terminate migraine headaches would act quickly, be highly efficacious, and have a low potential to cause critical adverse results. The newer serotonin agonists (triptans) seem to be less poisonous and barely simpler than the ergot preparations. The optimum use of abortive therapy requires prudent drug selection and affordable restrictions on drug use to avoid toxicity or habituation. The effectiveness of a given drug varies extensively from affected person to affected person, so a even handed trial of several medication is usually required to decide the simplest drug for a specific patient. To consider the results of drug remedy, the affected person should be instructed to hold an correct log of drug dosage and symptom severity, particularly throughout a trial interval. The overuse of abortive drugs can lead to serious toxicity, so patients should be properly instructed about limiting their use of these medication. According to the rules of the National Headache Foundation, sufferers ought to limit their use of ergotamine to 8 remedy days per month, with an ample interval between remedy days. They ought to restrict their use of sumatriptan and different triptan drugs to 6 therapy days per thirty days and a pair of treatment days per week, and they need to limit their use of opioid medicine to 2 treatment days per week. Pain typically lasts from 15 minutes to 3 hours and usually happens on the same time every day. The incidence of cluster headache dysfunction is low, nonetheless; it impacts less than 0. Drugs to forestall cluster complications embrace verapamil (see Chapter 11), and lithium (see Chapter 22). Other brokers which may be efficient in aborting cluster headaches embody inhaled oxygen, intranasal lidocaine, and glucocorticoids. Guidelines for selecting medication to handle cluster headaches are similar to these outlined previously for migraine headaches. This common sort of headache usually responds to physiologic approaches that appropriate cervical or dental alignment or visible refractive error. This drug is usually tolerated nicely when therapy is initiated with a low dose at bedtime, and the dosage is gradually elevated over a period of several weeks. They can be terminated with ergot alkaloids, sumatriptan, inhaled oxygen, intranasallidocaine,orglucocorticoids. A 35-year-old lady with a historical past of migraine reviews to her doctor that the final time she used her medication to stop an acute assault, she felt numbness and tingling in her extremities and blanching and cyanosis of her fingers. The triptan agents are efficient solely in the acute therapy of a migraine headache. Answers B by way of E have shown varied degrees of effectiveness in preventing migraines in controlled studies. Answers A and C via E are mechanisms of different brokers unrelated to the clinically used triptan medicine. Verapamil is used for the treatment of migraine or, better acknowledged, the prophylactic treatment to prevent migraine attacks due to its capability to block calcium channels and trigger vasodilation. Which of the following agents has not shown effectiveness in the prophylactic therapy of migraine headache Use of sumatriptan is contraindicated in which one of the following teams of sufferers The therapeutic effect of the triptan class of drugs is caused by which mechanism of motion Verapamil is indicated for the remedy of migraine as a end result of it has which one of the following results In addition, many patients have extraarticular manifestations, such as vasculitis, lymphadenopathy, and splenomegaly. Both humoral and mobile immune mechanisms are concerned within the pathogenesis of the disease. These mechanisms include the cytokine-mediated activation of T and B lymphocytes and the recruitment and activation of macrophages. The inflammatory leukocytes then release a selection of prostaglandins, cytotoxic compounds, and free radicals that cause joint irritation and destruction. Pathogenesis of rheumatoid arthritis Increased osteoclast activity and websites of action of selected antirheumatic drugs. In this simplified view of the immune system, dendritic (antigen-presenting) cells phagocytose antigens and current them to T cells, thereby activating the T cells. Methotrexate and leflunomide inhibit the proliferation and exercise of T cells and B cells. Eventually the cartilaginous layer is totally destroyed, leading to erosion and microfractures within the underlying bone. It is a sterile, viscoelastic solution ready from rooster combs (the fleshy growths on high of hen heads). The deposition of those crystals happens as a consequence of hyperuricemia, which might end result from overproduction or underexcretion of uric acid. Cancer chemotherapy can even increase plasma uric acid by cell dying and lysis, releasing purines into the plasma; the purines are subsequently catabolized to uric acid. Subsequent assaults of gout can be prevented by long-term therapy with a drug that either will increase uric acid excretion or inhibits uric acid formation and thereby reduces the serum stage of uric acid as discussed later. Prostaglandin Effects Prostaglandins play an necessary position in the growth of pain, inflammation, and fever. Prostaglandins are launched from cells in response to chemical stimuli or physical trauma. They sensitize sensory nerve endings to nociceptive stimuli and thereby amplify the technology of ache impulses. They additionally promote tissue irritation by stimulating inflammatory cell chemotaxis, causing vasodilation and growing capillary permeability and edema. This in flip prompts temperatureraising mechanisms, corresponding to a reduction in heat loss by way of cutaneous vasodilation, and causes the temperature to rise.
Order 40 mg isoptin otc
The traditionally proposed mechanism is a lower in heart fee and blood strain arteria umbilical unica consecuencias generic 240 mg isoptin amex, leading to xeloda arrhythmia cheap 240 mg isoptin with visa lowered cardiac oxygen demand, thereby optimizing oxygen balance and potentially decreasing infarct dimension. Generally speaking, -blockers should be considered in sufferers with a Killip score of 1 or 2, however must be avoided in those with a rating of 3 or 4. Statins, notably in high doses, seem to be useful within the setting of acute coronary syndrome. Patients appear to derive benefit whether the statin is started as a new treatment or continued prior statin therapy. Although extremes of glycemia seem to be deleterious, so too does makes an attempt at tight glycemic control. Benefits accrued by tight glycemic control may be outweighed by risk of hypoglycemia and a corresponding surge in adrenergic tone, with doubtlessly harmful results on the heart. Insulin remedy, when utilized, have to be administered prudently to avoid hypoglycemia. Hypoglycemia is related to elevated risk of cardiac death in critically sick sufferers. This affected person is at excessive risk for ventricular arrhythmias, supraventricular arrhythmias, and bradyarrhythmias. Ischemic and/or scarred myocardium presents a wonderful electrical substrate for life-threatening ventricular arrhythmias. In addition to making certain adequate revascularization, some easy maneuvers may help minimize the chance of ventricular arrhythmias. Second, correction of hypokalemia, hypomagnesemia, hypocalcemia, and acidosis are essential. Any arrhythmogenic inotropes such as catecholamines, dobutamine and milrinone should be stopped as soon as possible. Supraventricular tachycardias, although much less dangerous than ventricular arrhythmias, are extra widespread. Advanced age, hypertension, and systolic dysfunction are all thought to be danger factors. Adequate administration of electrolytes and acid/base abnormalities will also assist to forestall or decrease atrial arrhythmias. They are often transient, driven by increased vagal tone, and may generally be managed expectantly. Symptomatic sinus bradycardia will usually respond to atropine, and if it persists and is related to hypotension, dopamine may be an efficient short-term therapy. Ventricular arrhythmias may be prevented by use of -blockers, correction of electrolyte and acid/base abnormalities, and removal of inotropes. It is characterised by a harsh systolic murmur (sometimes with an related thrill) and shock. Ventricular free wall rupture is a devastating complication that presents suddenly with hemodynamic collapse and pericardial tamponade. Even for these in whom this condition is diagnosed rapidly, mortality rates are quite excessive. Bedside clues embody elevated jugular venous stress, pulmonary edema, cool extremities, altered psychological status, tachycardia, and hypotension. In such situations, new ischemia ought to be ruled out, and one must contemplate use of either inotropes or mechanical circulatory assist similar to intraaortic balloon pump as temporizing measures. A pulmonary artery catheter could also be useful in this state of affairs to monitor cardiac output and pulmonary artery oxygenation, and other invasive hemodynamics can be used to monitor response to therapy. Patients might current with little greater than delicate again ache, termed access site pain. Hypotension could additionally be exacerbated by concurrent vasovagal response, which is a standard response to access website ache and extended compression of the artery. This ought to be suspected within the setting of concurrent bradycardia and hypotension and should reply to atropine and/or dopamine. Bedside examination to consider for groin hematoma is essential, as is serial monitoring of complete blood depend. Care is above all supportive, requiring prolonged guide compression of the femoral artery and resuscitation with blood and intravenous fluids. The above situations can typically be rapidly excluded with a eager bedside examination and targeted echocardiogram. When doubtful, continued reassessment and exclusion of life-threatening circumstances will eventually convey a few diagnosis. Clinical examination and echocardiography are essential to quickly establish or exclude mechanical issues. The optimum duration of twin antiplatelet therapy depends on the clinical setting and the type of stent deployed. In the setting of stable coronary disease, the kind of stent dictates the length of remedy. The affected person needs to obtain anticoagulation therapy long run for atrial fibrillation. Concomitant atrial fibrillation also requires use of oral anticoagulation for stroke prevention. However, the usage of antithrombotic "triple remedy"-dual antiplatelet remedy plus oral anticoagulation-is related to a very high annual danger of major bleeding. After 1 yr, the double therapy arm had markedly lower charges of bleeding as nicely as a slight profit with respect to composite ischemic outcomes. These information recommend that sufferers who require twin antiplatelet remedy and anticoagulation could be managed safely in an aspirin-free regimen using clopidogrel and warfarin only. In medical expertise, some operators favor the usage of triple therapy for 1 month solely (to reduce risk of stent thrombosis), followed by warfarin and clopidogrel thereafter. There are little knowledge to information decision-making as regards to newer P2Y12 inhibitors and/or non-vitamin K antagonist oral anticoagulation. Clinically, the limited information are often closely extrapolated (eg, double remedy with clopidogrel and rivaroxaban), though reliable information are lacking for such newer brokers. Large, scientific trials are at present underway testing the security and efficacy of various remedy permutations in this setting, which is able to probably be the subject of ongoing analysis for a while. Prasugrel versus clopidogrel for acute coronary syndromes without revascularization. Adding heparin to aspirin reduces the incidence of myocardial infarction and dying in patients with unstable angina: a meta-analysis. Early intravenous beta-blockers in sufferers with acute coronary syndrome-a meta-analysis of randomized trials. Effect of statin use inside the first 24 hours of admission for acute myocardial infarction on early morbidity and mortality. Early risk of mortaliy after coronary artery revascularizatinon in sufferers with left ventricular dysfunction and potential position of the wearable cardioverter defibrillator. Proinflammatory cytokines in acute myocardial infarction with and without cardiogenic shock.
120 mg isoptin cheap free shipping
They stimulate protein synthesis in the brain and will thereby affect temper and emotions blood pressure medication grapefruit juice discount isoptin 240 mg without prescription. Estrogens influence the distribution of physique fats and thereby contribute to the event of feminine physique contours blood pressure medication that starts with a 120 mg isoptin discount with mastercard. They improve blood coagulation by rising the synthesis of clotting components, and so they prevent osteoporosis by inhibiting bone resorption. In men and women, estrogens are answerable for epiphyseal closure, which halts linear bone growth. They also affect the emotional state and have gentle mineralocorticoid (saltretaining) properties. Some of the synthetic progestins have other effects which may be attributed to their androgenic activity (see later). These cells present an setting wealthy in testosterone, which is important for germ cell development. Testosterone is answerable for the development of secondary intercourse characteristics in males during puberty. These include development of the larynx, thickening of the vocal cords, and development of facial, axillary, and pubic hair. In addition to stimulating growth of the penis, scrotum, seminal vesicles, and prostate gland, testosterone stimulates and maintains sexual perform in males. In this preparation, the quantity of estrogen (estradiol valerate) is sequentially stepped down during the administration cycle, whereas the quantity of progestin (dienogest) is stepped up. Conjugated equine estrogens are sulfate esters of estrone and equilin and can be obtained from the urine of pregnant mares. Micronized estradiol is an orally administered estradiol preparation that has good bioavailability. Also obtainable are vaginal estradiol tablets and a vaginal ring that slowly releases estradiol. Ethinyl estradiol and mestranol are modified by the addition of an ethinyl group to estradiol, which reduces firstpass metabolism, increases the half-life to about 20 hours, and results in greater oral efficiency compared with native estradiol. Conjugated equine estrogens are hydrolyzed to estrone and equilin earlier than absorption from the gut. They bear comparatively little first-pass metabolism and are converted within the liver to sulfate and glucuronide conjugates which might be excreted in the urine. Estrone is also out there in a rapidly absorbed formulation for intramuscular administration. Several long-acting formulations of estradiol are available for transdermal or intramuscular administration. Transdermal estradiol techniques slowly launch the drug for absorption via the skin. Estradiol cypionate and estradiol valerate are long-acting esters of estradiol which might be slowly absorbed after intramuscular administration and provide effective plasma concentrations of estradiol for Estrogens several weeks. Estradiol valerate can be contained in a variable dose oral contraceptive (Natazia), in which the estrogen dose is stepped up and the progestin dose is stepped down during each menstrual cycle. As with estrone and equilin, estradiol is metabolized in the liver to sulfate and glucuronide conjugates, and these conjugates are primarily excreted within the urine, with small amounts excreted within the feces. Estrogen preparations are used in the remedy of major hypogonadism, including circumstances attributable to surgical oophorectomy, menopause, and different causes. Combination estrogen-progestin preparations comprise both ethinyl estradiol or mestranol. These preparations are sometimes used for oral contraception and for the treatment of zits vulgaris and dysmenorrhea. A latest study found that oral estradiol valerate and dienogest successfully managed heavy or extended menstrual bleeding. Estrogens often trigger breast tenderness, headache, edema, nausea, vomiting, anorexia, and changes in libido. The extra serious opposed effects of estrogens embody hypertension, thromboembolic issues, and gallbladder disease. Estrogens improve ldl cholesterol excretion in the bile, accounting for his or her tendency to cause gallstones. Estrogens are contraindicated during being pregnant and ought to be avoided in ladies with uterine fibroids. Estrogens ought to be used with nice caution in women with hepatic diseases, endometriosis, thromboembolic illnesses, or hypercalcemia. Progesterone and Its Derivatives Progesterone is the primary pure progestin in mammals. Progesterone undergoes extensive first-pass metabolism after oral administration and has a short plasma half-life. To extend the oral bioavailability and half-life, esters of progesterone have been developed. These embrace megestrol, hydroxyprogesterone caproate, and medroxyprogesterone acetate. Megestrol is run orally, whereas hydroxyprogesterone caproate is run as a long-acting intramuscular preparation. Following their absorption, the progesterone esters are certain to albumin in the circulation. The esters are transformed to several hydroxylated metabolites and to pregnanediol glucuronide in the liver, and these metabolites are excreted within the urine. Progesterone esters are used to suppress ovarian operate in the remedy of dysmenorrhea, endometriosis, and uterine bleeding. In this setting the progesterone derivatives produce suggestions inhibition of gonadotropin secretion by the pituitary gland. Studies found that women treated with the drug had considerably fewer preterm deliveries. Most of the artificial progestins are derivatives of nortestosterone (testosterone and not utilizing a methyl group on carbon19) and have varying levels of estrogenic, antiestrogenic, and androgenic exercise. Norgestrel has extra androgenic activity than different progestins, whereas desogestrel and norgestimate have much less androgenic and more progestational activity. The synthetic progestins also contain molecular entities that increase their oral bioavailability and period of action. Their half-lives vary from 7 to 24 hours, whereas the half-life of progesterone is simply about 5 minutes. This is as a end result of giving estrogen alone increases the risk of endometrial most cancers in these ladies. Therapeutic Effects Studies constantly show that estrogens relieve symptoms of menopause in up to 90% of girls.
Isoptin 240 mg buy online
Dopamine launched in the nucleus accumbens is the ultimate widespread pathway for reinforcing drugs (and addictive behaviors) blood pressure numbers chart isoptin 240 mg order without prescription. Cocaine and amphetamines cause an elevated release of dopamine immediately at the nerve terminals within the nucleus accumbens blood pressure 35 weeks pregnant purchase isoptin 40 mg with amex. Drug Addiction Drug addiction usually refers to an extreme sample of drug abuse during which a person is repeatedly preoccupied with drug procurement and use and thus neglects different obligations and personal relationships. The time period addict has a pejorative connotation, nonetheless, and the trendy remedy of substance abuse as a illness state calls for use of the time period drug-dependent individuals or sufferers. Such sufferers are mentioned to have a substance abuse dysfunction, as outlined in the Diagnostic and Statistical Manual of Mental Disorders, used by psychiatrists. In many instances, individuals with a substanceabuse disorder are using authorized or unlawful substances as self-medication for comorbid disorders corresponding to nervousness or depression. After describing the pharmacologic results of these medicine and any medical use that they may have, this chapter discusses the remedy of substance abuse. Tables 25-1, 25-2, and 25-3 provide information about the manifestations and remedy of drug intoxication and withdrawal. Disulfiram inhibits aldehyde dehydrogenase and results in the buildup of acetaldehyde throughout ethanol ingestion. Fomepizole inhibits alcohol dehydrogenase and is utilized in methanol or ethylene glycol poisoning. In the United States alone, the price of health care, misplaced work hours, legal exercise, and different issues related to alcohol use is roughly $90 billion every year. The alcohols and glycols most commonly ingested are ethanol, methanol, and ethylene glycol. Ethanol has enough lipid solubility to enable speedy and nearly complete absorption from the intestine. It is more rapidly absorbed from the duodenum than from the abdomen, and meals slows its absorption by slowing the rate of gastric emptying. The acetate derived from ethanol enters the citric acid cycle for further oxidation to carbon dioxide and water. Because ethanol can markedly impair the psychomotor expertise required to safely drive a car, practically all nations prohibit the operation of motor vehicles while inebriated. The capacity of alcohol dehydrogenase to metabolize ethanol is proscribed because the enzyme is saturated at relatively low ethanol concentrations. Hence, ethanol metabolism reveals zero-order kinetics, except when serum concentrations of ethanol are very low. An adult weighing 70 kg often metabolizes only about 10 mL of absolute ethanol per hour, which is roughly equivalent to the quantity of ethanol contained in one alcoholic drink. It thereby produces sedative-hypnotic, anxiolytic, amnesic, and anticonvulsant effects. However, long-term ethanol use or ethanol withdrawal might lower the seizure threshold and thereby cause seizures. Ethanol at low doses produces disinhibition and gentle euphoria, which facilitate social interactions by lowering behavioral inhibitions and self-consciousness. In many individuals, reinforcement leads to the continued consumption of alcoholic beverages and to ethanol intoxication. This drawback is exacerbated by the restricted fee at which ethanol can be eliminated from the physique. Ethanol also inhibits the discharge of antidiuretic hormone from the pituitary gland and thereby produces a diuretic effect. This diuretic effect is augmented by the consumption of large volumes of alcoholic drinks, corresponding to a six-pack of beer. Ethanol produces vasodilation and will increase warmth loss from the body, partly by interfering with temperature regulation by the hypothalamus. Consumption of enormous quantities of ethanol on a long-term foundation can eventually lead to alcoholic cardiomyopathy and cardiac arrhythmias. In alcoholic patients, thiamine deficiency secondary to a poor food plan is commonly observed, which finally ends up in nerve demyelination. This, in turn, causes peripheral neuropathies, characterised by paresthesias and decreased sensory acuity. Thiamine deficiency can also cause Wernicke-Korsakoff syndrome, a behavioral disorder characterised by confusion, extreme anterograde and retrograde amnesia, ataxia, nystagmus, and ophthalmoplegia. The administration of thiamine substantially reverses all but the amnesic effects seen in sufferers with this syndrome. A dietary deficiency of folate can result in megaloblastic anemia, whereas a deficiency of other vitamins and antioxidants contributes to the general tissue damage observed in alcoholism. The consumption of great portions of ethanol throughout being pregnant is answerable for the occurrence of the fetal alcohol syndrome, which is characterised by low delivery weight, microcephaly, facial abnormalities (flattening), psychological retardation, coronary heart defects, and other abnormalities. Other Alcohols and Glycols Methanol, also called methyl alcohol or wooden alcohol, is a highly toxic type of alcohol that can trigger profound anion hole metabolic acidosis and severe damage to the eyes. Formate is primarily responsible for optic nerve injury, which can lead to visible field impairment or permanent blindness. In circumstances of methanol poisoning, sufferers are handled with ethanol, which serves to saturate alcohol dehydrogenase and thereby prevent the formation of formaldehyde and formate. Fomepizole, an inhibitor of alcohol dehydrogenase, may also be administered; this prevents the formation of toxic metabolites in instances of methanol and ethylene glycol poisoning. Isopropyl alcohol is transformed to acetone, a substance that could be smelled on the breath. Owing to its candy style and appealing shade, kids typically die from ethylene glycol poisoning from car antifreeze left accessible in the storage. Ethylene glycol is metabolized to oxalic acid, and calcium oxalate crystals may be found within the urine of patients after ethylene glycol ingestion. Treatment consists of supporting vital capabilities, giving ethanol or fomepizole, managing acidosis, and performing hemodialysis. The pharmacologic properties of barbiturates and benzodiazepines are mentioned in Chapter 19. These medication are sedative-hypnotic agents which might be prescribed for the therapy of anxiety issues, insomnia, and different conditions. They are used recreationally for his or her euphoric and anxiolytic effects, and a few polydrug users use them to cut back the irritability and anxiousness associated with cocaine or amphetamine use. Flunitrazepam has gained notoriety as a party drug, a club drug, and a drug that contributes to date rape. Flunitrazepam produces drowsiness, impaired motor skills, and anterograde amnesia. The long-term use of barbiturate or benzodiazepine drugs can result in psychological and physical dependence, and their abrupt withdrawal produces signs that are just like those brought on by alcohol withdrawal (see Table 25-3). It can also be listed by the Drug Enforcement Administration as a predatory or date-rape drug.
Isoptin 240 mg buy visa
The nitrosourea drugs embrace carmustine (bis-chloroethyl nitrosourea) pulse pressure variation ppt generic isoptin 120 mg online, lomustine (cischloroethyl nitrosourea) arteria magna discount 240 mg isoptin, and a intently associated methylnitrosourea called streptozocin. The nitrosoureas are bifunctional alkylating medicine with structures much like those of the nitrogen mustards. They are extremely lipophilic and attain cerebrospinal fluid concentrations which would possibly be about 30% of plasma concentrations. Both medication are used to treat lymphomas, and carmustine is also used to treat melanoma and a quantity of myeloma. Streptozocin is used only to deal with carcinoid tumor and pancreatic islet cell tumor (insulinoma). The nitrosoureas produce delayed and prolonged myelosuppression, with complete recovery taking 6 to 8 weeks. The thrombocytopenia caused by nitrosoureas normally happens earlier and is extra pronounced than the leukopenia produced by these medication. Although all the medicine cause nausea and vomiting, these effects are most pronounced with streptozocin therapy. The medication cisplatin, carboplatin, and oxaliplatin are inorganic platinum derivatives. This leads to the formation of intrastrand cross-links between neighboring guanine residues. Cisplatin produces delicate myelosuppression but may cause severe nausea, vomiting, and nephrotoxicity. The use of mannitol and sodium thiosulfate will decrease the severity of nephrotoxicity, an antagonistic effect associated with loss of potassium and magnesium, lowered glomerular filtration, and renal failure. Mannitol will increase urine move and can cut back binding of cisplatin to renal tubule proteins. Sodium thiosulfate accumulates in renal tubules and neutralizes the cytotoxicity of cisplatin. Busulfan is an alkyl sulfonate drug that acts as a bifunctional alkylating agent in the same manner as the nitrogen mustards act. Unlike other alkylating medication, busulfan has greater activity in opposition to myeloid cells than against lymphoid cells. Busulfan causes delicate nausea and vomiting and produces dose-limiting myelosuppression. It also can trigger pulmonary fibrosis ("busulfan lung"), which happens in about 4% of sufferers handled on a long-term foundation with the drug. It is characterised by a nonproductive cough, dyspnea, and a reticular pattern on chest x-ray film. No therapy has been successful, and the typical survival after prognosis is 5 months. After parenteral administration, the drug is activated by hepatic discount reactions to the active alkylating compound. Mitomycin is used for abdomen and pancreatic most cancers and in the therapy of transitional cell carcinomas of the bladder. Mitomycin produces delayed and prolonged myelosuppression that preferentially affects platelets and leukocytes. It also can cause pulmonary damage as well as hemolytic anemia and renal dysfunction. Temozolomide is a first-line drug for a quantity of mind tumors, together with astrocytoma and gliomas. Several of the medicine have a broad spectrum of activity in opposition to hematologic 471 cancers and strong tumors, whereas others have a more limited range of scientific uses. Daunorubicin and doxorubicin are antibiotics obtained from a Streptomyces species, and idarubicin is a semisynthetic derivative. Two of the four rings are quinone and hydroquinone moieties that allow the compounds to accept and donate electrons and thereby promote the formation of free radicals. They avidly bind to tissues and have large volumes of distribution and lengthy half-lives. The medication are extensively metabolized within the liver, and a few metabolites are as pharmacologically energetic as the father or mother compounds. Daunorubicin and idarubicin are agents used in induction and consolidation remedy for acute myeloid leukemia. Among the antagonistic results of anthracyclines are myelosuppression and cardiac harm, which are dose-limiting results; nausea and vomiting, which are doserelated and may be moderate to extreme; alopecia; and mucosal ulcerations. Extravasation of the medication during intravenous infusion can result in extreme localized tissue ulceration and necrosis. These localized reactions can progress over many weeks, and no effective remedy for them at present exists. Hence, distinctive care and specialized coaching are required for proper administration of anthracycline drugs. Manifestations of acute toxicity embrace sinus tachycardia and ventricular premature beats. These cardiac rhythm disturbances typically occur in the course of the first 24 hours and are self-limited. Chronic toxicity leads to congestive cardiomyopathy and limits the cumulative dose of anthracycline that can be given to any patient. The cardiomyopathy appears to end result from iron-catalyzed formation of free radicals. Information about this course of has led to the development of a cardioprotective drug referred to as dexrazoxane. Dexrazoxane is primarily given to women with breast most cancers who might benefit from continued doxorubicin remedy. Drugs that improve the toxicity of doxorubicin include cyclosporine, cyclophosphamide, and mercaptopurine. Verapamil can increase the cytotoxicity of doxorubicin and different anthracycline drugs by inhibition of the Pgp that transports anthracyclines out of cells. Partly for that reason, mitoxantrone causes much less cardiotoxicity, much less tissue harm after extravasation, and less nausea, vomiting, mucosal ulceration, and alopecia than do doxorubicin and other anthracycline antibiotics. The drug has its biggest effect on neoplastic cells in the G2 section of the cell replication cycle. Bleomycin is administered intravenously, is broadly distributed, and is primarily eradicated by renal excretion. The drug is inactivated in cells by aminohydrolase, whose low ranges in skin and lung could partly account for the toxicity of bleomycin in these tissues. Bleomycin has a broad range of exercise and is certainly one of the most widely used antitumor antibiotics. It is helpful in Hodgkin and non-Hodgkin lymphomas, testicular cancer, and several other different solid tumors.
Isoptin 240 mg without a prescription
Group three had the highest incidence of vasospasm blood pressure medication history safe isoptin 120 mg, however different teams additionally had vasospasms hypertension treatment guidelines 120 mg isoptin effective, simply much decrease in frequency. There have been concerns within the literature reporting a low correlation between the Fisher grade and the incidence of symptomatic vasospasm (one latest study showed about 50% correlation between the Fisher grade and vasospasm). Effect of cisternal and ventricular blood on danger of delayed cerebral ischemia after subarachnoid hemorrhage: the Fisher Scale revisited. In order to decrease the interobserver variability in assessing the estimated volume of blood in the subarachnoid space, a volumetric quantification of Fisher grade three has been proposed and studied by Friedman and colleagues from the Mayo Clinic. Quantitative evaluation of hemorrhagic quantity for predicting delayed cerebral ischemia after subarachnoid hemorrhage. Over the final 30 years, it has turn into clear that the larger the amount of blood within the basal cisterns, the larger the chance of vasospasm. To evaluate this danger, varied grading schemes have been proposed, from easy to elaborate, probably the most extensively identified being the Fisher scale. Most just lately, volumetric quantification and clearance models have provided essentially the most detailed analysis. Angiography shows an anterior communicating (A-comm) artery aneurysm, and coiling was carried out to secure the ruptured aneurysm. This is a advice that displays the newest medical treatment obtainable within the literature. Decompressive craniectomy/craniotomy is the simplest way of reducing intracranial hypertension. Step 1: Sedation with Short-Acting Agents (Patients ought to be on mechanical ventilation. Analgesia is an important step in managing intracranial hypertension if pain is suspected as a element of agitation. Shivering prevents the core physique temperature from falling and results in prolonged time to achieve the goal temperature. Increased cerebral blood quantity might lead to any one of the following eventualities: 1. Development of vasoconstriction would occur if autoregulation is unbroken in response to increased blood quantity delivered. No vasoconstriction would occur if autoregulation is impaired (pressure�volume breakdown). A combined picture of all the above as completely different components of the mind have both impaired or intact autoregulation at a degree previous to the pressure�volume breakdown. The oxygen content material within the venous return from the brain again to the center (measured by Sjvo2) depends on the Do2 and oxygen consumption (Vo2). As the consumption of oxygen decreases, the extraction decreases as not as a lot oxygen is required to be extracted from the vasculature into the mind cellular tissues. Understanding this relationship is essential in making use of this principle to the bedside data. What may you do to improve the brain oxygenation and scale back the brain metabolic stress There are ongoing debates relating to whether the partial pressure of oxygen pressure measured within the brain means anything in brain-injured sufferers (or what it means within the short or long term). Frequently encountered criticisms are focused on the reality that the location of the probe is probably not in the good location for monitoring the injury. The probe provides direct information, however it solely supplies the native information, and the quantity it gives may not be relevant to the rest of the mind. It is also criticized that the absolute value of Pbto2 could not always correlate with the long-term end result, making it troublesome to determine what the crucial or "harmful" worth is. Another factor, mind mobile metabolism, plays a role in determining the Pbto2 as it influences the consumption and extraction of the delivered oxygen supply. This false rate then results in more pointless and probably dangerous interventions. The cerebral ischemic cascade is advanced, and the compensatory mechanisms, within the setting of ischemia due to vasospasm, result in a variety of scientific findings: from normal to focal deficit. This is the window of opportunity for appropriate medical and endovascular interventions. Despite the small sample sizes, research report a somewhat excessive positive predictive value and a false-negative rate. The patient becomes acutely left hemiparetic with further depressed level of arousal on bleed day 7. A longer delay in getting the angiogram leads to a better threat of irreversible ischemic damage. Hypertensive Euvolemic Therapy Triple-H remedy has been used for many years to enhance and keep enough brain perfusion in sufferers with symptomatic vasospasm. This should be emphasised even more within the event of cerebral vasospasm and delayed cerebral ischemia as intravascular volume depletion might considerably contribute to devastating ischemic injuries. In that examine, the rate of developing symptomatic vasospasm was the identical for both hypervolemic and normovolemic teams. Until there are a quantity of randomized studies confirming what should be the gold commonplace, clinicians should be treating the patients with the most effective available knowledge, proof, and, most of all, good judgment (because knowledge and evidence-based medical literature alone are often not adequate to make a good decision). The following is a reasonable algorithm for managing patients with danger of developing symptomatic vasospasm and delayed cerebral ischemia. Symptomatic vasospasm is a time-sensitive emergency, and well timed treatment with balloon angioplasty inside 2 hours of symptom onset has been proven to produce sustained medical enchancment. Hence, within the absence of different intrinsic renal disease as a confounder, an sufficient urine output is a reasonable hemodynamic management target to "optimize" medical therapy for sufferers with symptomatic vasospasm. A variety of totally different combos of these agents are getting used intraarterially in patients all over the world. Conventional cerebral angiography shows extreme right-sided inside carotid artery vasospasm in the carotid terminus. If the patient has aspiration pneumonia and is on a high-maintenance ventilator setting with multiple vasopressors, the presence of an anesthesiologist is needed for subsequent remedies, and this may be one other source of delay. It is troublesome to quantify how lengthy these vasodilators may work as every affected person responds differently. Every practitioner has different thresholds for choosing totally different strategies to tackle severe vasospasm. Given anecdotal stories of optimistic findings in both preventing and treating vasospasm, additional studies are warranted to investigate the safety and efficacy of this remedy. As more PbtO2 and different multimodality brain-monitoring probes are used in clinical practice, there could also be more details about how intraventricular use of vasodilators may enhance the cerebral blood flow and whether it has more influence on the proximal versus distal vasculature. The implant group had a considerably reduced incidence of angiographic and symptomatic vasospasm with better short- and long-term end result. Despite rather convincing knowledge, you will want to keep in mind that this therapy requires surgical clipping of the aneurysm and thorough washout of the recent blood clots, adopted by multiple implantation of nicardipine pellets.
Diseases
- Glycogen storage disease type VIII
- Glucagonoma
- Uveitis, anterior
- Coarse face hypotonia constipation
- Scalp ear nipple syndrome
- Lecithin cholesterol acyltransferase deficiency
- Pseudo-Zellweger syndrome
- Chromosome 16, uniparental disomy
- Coffin Lowry syndrome
- Weaver-like syndrome
Isoptin 120 mg generic mastercard
The administration of plasma glucose in acute cerebral ischaemia and traumatic brain injury: extra analysis needed blood pressure j curve 240 mg isoptin quality. Safety and feasibility of intra-arterial nicardipine for the treatment of subarachnoid hemorrhage-associated vasospasm: initial scientific expertise with high-dose infusions pulse pressure 12080 isoptin 120 mg cheap line. High-dose intraarterial verapamil in the treatment of cerebral vasospasm after aneurysmal subarachnoid hemorrhage. Intraarterial nimodipine for the therapy of symptomatic cerebral vasospasm after aneurysmal subarachnoid hemorrhage: preliminary outcomes. Preliminary experience with intra-arterial nicardipine as a therapy for cerebral vasospasm. Cerebral arterial spasm-a controlled trial of nimodipine in patients with subarachnoid hemorrhage. Intensive insulin remedy reduces microdialysis glucose values without altering glucose utilization or bettering the lactate/pyruvate ratio after traumatic mind harm. Insulin-related lower in cerebral glucose regardless of normoglycemia in aneurysmal subarachnoid hemorrhage. Systemic glucose variability predicts cerebral metabolic misery and mortality after subarachnoid hemorrhage: a retrospective observational research. Striking variations in glucose and lactate levels between brain extracellular fluid and plasma in conscious human topics: effects of hyperglycemia and hypoglycemia. Transient focal increase in perihematomal glucose metabolism after acute human intracerebral hemorrhage. The glucose transporter household: structure, perform and tissue-specific expression. Cerebral hyperglycolysis following extreme traumatic brain injury in humans: a positron emission tomography research. Continuous monitoring of regional cerebral blood flow: experimental and clinical validation of a novel thermal diffusion microprobe. Effect of intra-arterial papaverine on regional cerebral blood flow in hemodynamically related cerebral vasospasm. Continuous monitoring of regional cerebral blood move throughout temporary arterial occlusion in aneurysm surgery. Jugular bulb oximetry for prediction of vasospasm following subarachnoid hemorrhage. Fever after aneurysmal subarachnoid hemorrhage: relation with extent of hydrocephalus and amount of extravasated blood. Cortical spreading ischaemia is a novel course of concerned in ischaemic injury in patients with aneurysmal subarachnoid haemorrhage. Spreading depolarizations and late secondary insults after traumatic brain injury. Spreading depolarisations and end result after traumatic brain damage: a potential observational examine. Preliminary proof that ketamine inhibits spreading depolarizations in acute human mind damage. He is given fluid resuscitation with the infusion of 2 L of crystalloids, and blood stress recovers to 140/80 mm Hg. Although the aneurysm is unsecure, systemic hypertension must be prevented; nonetheless, hemodynamic stability is crucial to keep away from cerebral hypoperfusion, acute ictal infarcts, and cerebral circulatory arrest. Although frequently hypertensive, patients are admitted with relative intravascular volume depletion-due to natriuresis and the systemic inflammatory response related to severe brain injury-and 2 L of regular saline is acutely administered to preserve organ perfusion. At this point, urine output, central venous stress, arterial lactate levels, and central venous oxygen saturation (Scvo2) are assessed to refine the analysis of hemodynamic stability. Poor-grade subarachnoid hemorrhage (modified Fisher 3) caused by a proper internal carotid artery aneurysm rupture. The patient is submitted to cerebral angiography that reveals an aneurysm within the intracranial part of the proper inner carotid artery. A comprehensive method to goal-directed interventions requires that organ operate is assessed to indicate the need and evaluate the response to specific treatments. Our method to multimodal monitoring focuses on systemic and cerebral parameters and the interrelation between them, as proven in Table 17-1. Hemodynamic monitoring is a cornerstone of the administration of critically ill neurologic sufferers. The intracranial modalities are normally used as a bundle, inserted into a multilumen bolt, and/or tunneled in, as needed. Pbto2 is a measure of tissue oxygen rigidity and is believed to replicate the stability between delivery, consumption, and tissue diffusion of oxygen. Systemic hemodynamic resuscitation should at all times precede brain-targeted interventions. After hemodynamic stabilization, end-organ perfusion parameters ought to be reassessed. The goal of superior neuromonitoring in patients with extreme brain damage is to enable early detection of complications and ensure adequate delivery of oxygen and nutrients to the mind to be able to avoid everlasting harm. These probes are launched at the bedside via a multilumen bolt and/or are tunneled in subcutaneously. All the info are constantly displayed and saved at the bedside along with systemic monitoring parameters. An integrative strategy to mind oxygenation, metabolism, electrical exercise, and perfusion allows the clinician to understand the pathophysiology of occasions and to individualize scientific remedy. Early treatment to optimize perfusion may reverse these alterations and avoid a vasodilatory cascade that leads to refractory intracranial hypertension. Taking into account the complexity and interactions between these variables, efforts are undertaken to regulate sedation, serum osmolarity, and blood glucose control and exclude surgical problems via neuroimaging whereas hemodynamics are optimized. Supranormal goals are defined as optimal if they correlate with improvements in the cerebral oxygenation and metabolic profile. An echocardiogram performed 2 days earlier revealed a reasonable left ventricular24 dysfunction, and most troponin ranges of 4 was reached on post-bleed day 2. Neurocritical Care Monitoring What must be the approach to a affected person with suspected vasospasm and myocardial dysfunction Those who present with diffuse and thick cisternal blood are especially at increased threat for delayed infarcts due to vasospasm. There is increasing proof that multimodality monitoring allows early detection of cerebral ischemia due to vasospasm before clinical indicators develop. Angiography and definite therapy with intraarterial vasodilators and balloon angioplasty are often essential for refractory symptomatic vasospasm. Cerebral angiography (top left) shows vasospasm of the proper middle cerebral and anterior cerebral arteries. The second radiograph demonstrates a model new proper decrease lobe infiltrate that advanced into a ventilator-associated pneumonia. Extreme caution to keep away from pointless fluid overloading is warranted through the course of fluid resuscitation. We choose utilizing fluid boluses of crystalloid as wanted instead of continuous infusion of huge volumes of fluid. Ineffective fluid challenges will fail to increase cardiac output, and thus cerebral blood move, and contribute to pulmonary edema.
40 mg isoptin generic otc
The parenterally administered agonistantagonist drugs are primarily used for preoperative and postoperative analgesia and for obstetric analgesia during labor and delivery arteria espinal anterior order 120 mg isoptin otc. The orally and nasally administered medication are used to alleviate moderate to extreme ache blood pressure medication causing dizziness isoptin 40 mg discount with amex. Specific Drugs Buprenorphine, which is a partial agonist at � receptors, is famous for a gradual dissociation from the � opioid receptor after binding. It is somewhat longer appearing than most parenterally administered opioid analgesics and may be administered intramuscularly or intravenously. It was recently approved for outpatient therapy of opioid dependence (see Chapter 25). It is out there in an oral and sublingual formulation mixed with naloxone (as Suboxone) to stop intravenous abuse. Butorphanol and nalbuphine, which are opioid receptor agonists, have partial agonist or antagonist exercise at � opioid receptors. Both drugs are administered parenterally, and butorphanol can additionally be obtainable as a nasal spray. Pentazocine is a opioid receptor agonist with further activity at (sigma) receptors. The parenteral formulation is primarily used as a preanesthetic treatment and as a complement to surgical anesthesia. The oral formulations are used to deal with reasonable to extreme pain, and certainly one of them contains naloxone, a pure opioid antagonist, to discourage parenteral abuse of the drug. Parenteral use of an oral pentazocine formulation can cause severe cardiovascular effects, especially in sufferers with existing cardiovascular disease. Pentazocine is also obtainable in combination with aspirin or acetaminophen for oral administration. Mixed Opioid Agonist-Antagonists and Partial Agonists the mixed opioid agonist-antagonists are drugs that exhibit partial agonist or antagonist activity at � receptors and show agonist or antagonist exercise at receptors. The blended opioid agonist-antagonists have a large chemical group on the nitrogen atom of the morphine molecule, which is answerable for their partial agonist or antagonist activity at opioid receptors. In addition, pentazocine is out there for oral use and butorphanol is out there as a nasal spray. Butorphanol is rapidly absorbed from the nasal mucosa, which thereby enables the use of the drug on an as-needed basis. The most necessary pharmacologic property of those medication with respect to their medical activity is the shortage of full agonist effects at � opioid receptors. Because of this, the mixed opioid agonist-antagonists produce much less respiratory depression as the doses are elevated than do strong opioid agonists similar to morphine. Hence, the blended opioid agonist-antagonists are safer to use with regard to respiratory despair and overdose. They Opioid Antagonists Naloxone and naltrexone are competitive opioid receptor antagonists that may quickly reverse the effects of morphine and different opioid agonists. These pure opioid antagonists have two main clinical uses: the therapy of opioid overdose and the treatment of alcohol and opioid dependence. Naloxone and naltrexone are chemical analogues of morphine, with cumbersome chemical groups attached to the morphine molecule. This modification allows the molecule to bind to the opioid receptor however prevents the conformation change within the receptor required for agonist activity. In cases of opioid overdose, naloxone is run intravenously to quickly terminate respiratory depression and different poisonous effects of opioid agonists. Naloxone can additionally be formulated with opioid agonists in oral medications to prevent crushing of the pill and intravenous abuse. Naltrexone, in an oral formulation (ReVia) and in an extended-release injectable suspension (once-a-month, Vivitrol), can also be used to treat alcohol and opioid dependence. Acute Pain the location, trigger, and severity of pain and the chance of producing drug dependence are all elements that affect the way in which during which ache is managed. As a common rule, sufferers with acute or persistent pain should be treated with the least potent analgesic that will management their pain. Moderate to severe ache is commonly treated with codeine, hydrocodone, or oxycodone alone or in combination with a nonopioid analgesic. Acute pain caused by trauma, surgical procedure, or short-term medical circumstances may be successfully managed with an analgesic and acceptable remedy of the underlying condition. In patients with acute ache, the chance of manufacturing drug dependence is extraordinarily low. Pain associated with arthritis, neuropathy, and other persistent however nonterminal conditions is more difficult to deal with and is often managed with a mixture of analgesics, coanalgesics, psychotherapy, bodily therapy, and different therapy modalities. Use of opioid analgesics within the therapy of persistent ache is associated with a risk of opioid tolerance and physical dependence, so care should be exercised to forestall dosage escalation, drug dependence, and prescription drug abuse. Strict tips for prescription refills must be in place, and a prescription refill flowchart can be used to monitor drug utilization and prevent dosage escalation. In some clinics, patients are requested to sign an "opioid contract" in which they agree to procedures that can ensure correct use of opioid medication, together with random drug testing. Patients with terminal sicknesses, corresponding to metastatic most cancers, ought to obtain sufficient doses of opioid analgesics to management their ache, no matter any concerns concerning the improvement of tolerance and bodily dependence. Therefore in the initial levels of acute ache, analgesics ought to be given around the clock at regular intervals. The dosage should be titrated to control pain while minimizing sedation and other unwanted effects. As the ache subsides over time and the need for analgesia decreases, the patient can be transferred to an as-needed schedule of medicine. Patient-controlled analgesia is a technique of intravenous administration that permits the patient to self-administer preset amounts of an analgesic. Although the dialogue of specific persistent ache syndromes is past the scope of this text, a quantity of general tips and comments might be offered. Both opioid analgesics and nonopioid analgesics are useful in the management of chronic pain syndromes. If pain is related to irritation, nonopioid drugs with antiinflammatory exercise may be particularly helpful. If ache is related to peripheral nerve or nerve root sensitization, treatment with transcutaneous nerve stimulation or a local anesthetic might assist. Capsaicin produces a burning sensation for the first few days of application, but that is progressively changed by an analgesic impact. Recently a capsaicin patch formulation (Qutenza) was permitted for remedy of pain caused by postherpetic neuralgia. When ache has been present for a time frame, the responsiveness of dynamic widerange nociceptive neurons within the spinal wire increases in a method that increases ache notion and reminiscence.
Order isoptin 40 mg with visa
A man treated for a Nocardia asteroides infection subsequently develops hemolytic anemia blood pressure medication for dogs isoptin 40 mg buy on line. It results from infection of the skin and peripheral nervous system with Mycobacterium leprae arrhythmia junctional isoptin 120 mg purchase free shipping. Because this organism grows so slowly, the disease displays a gradual, progressive course over a number of a long time. The disease happens in two main types, lepromatous leprosy and tuberculoid leprosy, each of which has a attribute pathophysiology and clinical presentation. Treatment of leprosy can require years of remedy with antimycobacterial agents, though the introduction of newer medicine has enabled the utilization of shorter courses of remedy for many sufferers. There is an urgent want for novel brokers which are energetic against persistent organisms and thereby shorten the course of therapy. Hehasahistoryof knife wounds and was jailed for three months after a barroom fight 2 years in the past. His chest radiograph shows patchy infiltratesinbothupperlobes,andasputumsampleisfoundto containacid-fastbacilli. Thedefinitivediagnosisis based on finding acid-fast bacilli in sputum and a optimistic tuberculintestresult. First-line drugs are discussed later, and some of their properties are proven in Table 41-1. They include rifabutin and rifapentine (other derivatives of rifamycin), fluoroquinolone medicine (see Chapter 40), cycloserine, capreomycin, ethionamide, amikacin, and aminosalicylic acid. Isoniazid Isoniazid was developed after studies discovered that nicotinic acid had a weak antitubercular impact. The drug is extensively distributed to tissues and reaches intracellular concentrations sufficiently excessive to be efficient in opposition to organisms inside cells and caseous lesions. The major metabolite, acetylisoniazid, is formed by conjugation of acetate with isoniazid in a reaction catalyzed by acetyltransferase, an enzyme whose activity is genetically determined. Slow acetylation is an autosomal recessive trait, and individuals with the sluggish phenotype are homozygous for the sluggish allele. Because of the completely different rates of acetylation of isoniazid, persons with the quick phenotype have lower plasma isoniazid concentrations than do persons with the sluggish phenotype. The slow phenotype predominates in some Middle Eastern populations, whereas the quick phenotype predominates in Japanese populations. A small quantity of acetylisoniazid is transformed to isonicotinic acid and acetylhydrazine. Investigators believe that acetylhydrazine is answerable for the hepatic toxicity of the drug. This fatty acid is the mycobacterial cell wall part responsible for the acid-fast staining property of mycobacteria. Plasma concentrations of isoniazid had been measured 2 hours after the administration of a single 300-mg dose of isoniazid to each member of a general inhabitants of human topics. Subjects with the quick acetylation phenotype confirmed decrease plasma drug concentrations than did topics with the sluggish acetylation phenotype. Chapter 41 y Antimycobacterial Drugs growing organisms and protracted nongrowing (stationary phase) micro organism. Isoniazid, along with rifampin and pyrazinamide, eradicates rapidly growing organisms through the first 2 months of remedy. During the next 4 months of treatment, isoniazid and rifampin act in opposition to persistent bacteria that slowly revert to actively growing types. This resistance is mediated primarily by mutations of the katG gene that lead to loss of the catalase-peroxidase enzyme required for activation of isoniazid. Isoniazid is fairly well tolerated by most patients, however it causes elevation of serum transaminase levels and probably life-threatening hepatitis in some individuals. The danger of developing hepatitis during isoniazid therapy is low in individuals beneath 35 years of age, is moderate in persons aged 35 to 50 years, and is highest in individuals over 50 years of age. Isoniazid can also cause peripheral neuritis, with symptoms together with paresthesias and numbness of the fingers and toes. Peripheral neuritis is brought on by a pyridoxine (vitamin B6) deficiency ensuing from direct inactivation of pyridoxine by the drug. Hematologic abnormalities, corresponding to granulocytosis, anemia, or thrombocytopenia, can occur. Ethambutol Ethambutol is a butanol (butyl alcohol) by-product that has bacteriostatic exercise in opposition to mycobacterial organisms. Ethambutol is run orally, undergoes hepatic biotransformation, and is excreted within the urine and feces. The drug is mostly properly tolerated, however it could produce 427 dose-dependent optic neuritis and impaired red-green color discrimination. Including pyrazinamide in initial treatment regimens made it potential to reduce the treatment length to 6 months, whereas different therapies required 9 to 12 months. Pyrazinamide is normally given together with isoniazid, rifampin, and ethambutol (see Table 41-2). Pyrazinamide is given orally, is broadly distributed to tissues, and is basically converted to pyrazinoic acid within the liver. A small quantity of the drug is excreted unchanged within the urine, together with its metabolite. Adverse reactions to pyrazinamide embody arthralgia, hyperuricemia and gout, hematologic toxicity, fever, hepatitis, and a rise within the serum iron focus. Rifampin (also known as rifampicin) is a derivative of the antibiotic referred to as rifamycin that has improved pharmacokinetic properties compared with the pure antibiotic. Rifampin is rapidly absorbed after oral administration and is transformed within the liver to an lively metabolite, desacetyl-rifampin. The drug and its metabolite are extensively distributed to tissues and fluids, including lung tissue, saliva, and peritoneal and pleural fluids. It is primarily excreted within the feces by way of biliary elimination, but as a lot as 30% is excreted within the urine. Rifampin is a broad-spectrum antibiotic that has vital activity in opposition to many gram-positive, gram-negative, and acid-fast bacilli, including M. As with rifampin, rifabutin induces cytochrome P450 enzymes and may reduce serum concentrations of medication metabolized by these enzymes. The major drawback of rifampin is the tendency for microbes to acquire resistance throughout publicity to the drug. The adverse effects of rifampin are usually mild, but the drug can impair liver function, elevate serum bilirubin and transaminase ranges, and trigger hepatitis. Liver perform tests should be conducted each 2 to four weeks during remedy, and rifampin should be discontinued if indicators or symptoms of hepatic dysfunction become evident.
Quality isoptin 240 mg
If that is achieved with a nonprotective lung ventilation technique prehypertension causes symptoms 240 mg isoptin safe, the patient should be managed with the bottom tidal volumes and airway pressures possible heart arrhythmia xanax purchase isoptin 240 mg otc, and each attempt should be made for the most secure ventilatory technique as soon as attainable. His central venous strain is now 8 mm Hg, his distinguished V wave is gone, and repeat echocardiography after your interventions reveals improved perform of the right ventricle. Barotrauma represents extra-alveolar air from pneumothoraces, pneumomediastinum, subcutaneous emphysema, pneumoperitoneum, and pulmonary interstitial emphysema. Re-opening occurs with each inspiratory cycle, and this repetition is injurious to alveoli, inflicting shear injury. Alveolar epithelial damage, capillary endothelial damage, and diffuse pulmonary edema can occur. Barotrauma, atelectrauma, and volutrauma all doubtless lead to some extent, biotrauma. Encephalopathy and important illness polyneuropathy are properly described within the literature. This is regardless of the known neurologic problems of mechanical ventilation present within the literature for years and the extracranial problems of acute brain damage being well known. Also, sufferers with acute neurologic injury regularly current with pre-existing comorbidities. Given these details, a paradigm shift should occur as a result of no affected person should be considered to have "isolated head harm. Multiple research present persistent cognitive deficits that exist years after liberation from mechanical ventilation. If monitored with an esophageal balloon, transalveolar strain ought to be restricted to at least < 25 cm H2O. Brain-injured patients may profit from continuous brain tissue oxygen monitoring, and optimization of mind oxygenation must be thought of a potential goal of therapy. When appropriate and protected, all patients ought to be woke up every day, have daily spontaneous breathing trials, have targeted sedation to allow appropriate limitation of sedative infusions and limited benzodiazepine exposure, and be monitored for delirium. You would prefer to not intubate this affected person and surprise about using noninvasive constructive pressure air flow. It may be accomplished using a facemask or nasal masks fitted to the face and linked through standard ventilator tubing to both a normal mechanical ventilator or smaller ventilators made specifically to deliver noninvasive mechanical ventilation. Delivered tidal quantity relies on affected person effort, as nicely as the mechanics of the respiratory system. Your attending asks: "What are a few of the concerns to approaching mechanical air flow in patients with obstructive airway illness and expiratory circulate limitation Regardless of the precise illness that brought on the pathology, the increase in airway resistance, lack of regular lung elastance, and airway narrowing result in alveolar regions that have problem emptying and returning to resting endexpiratory lung volume, as nicely as increased inspiratory muscle workload. By elevating intrathoracic pressure and therefore right atrial strain, venous return may be impaired. In distinction to parenchymal pathology, the ventilationperfusion mismatch is one largely of increased useless space, as opposed to shunt. These modifications are in distinction to the patient with alveolar edema and consolidation, parenchymal pathology, and reduced compliance. The major etiology of respiratory failure is sort I, with hypoxia driven by shunt physiology. Instead, fundamental data of mechanical ventilation and physiologic rationale helps guide therapy and patient response. Expiratory time can also be extended by reducing tidal quantity and increase circulate price (in volume-targeted ventilation), but the clinician ought to be conscious that that is much less efficient, and an elevated circulate rate ends in elevated airway stress. For a breath to occur, a strain gradient should be overcome from the ventilator to the patient. However, despite a lower in minute ventilation, if this technique permits for decreased dead house, then air flow may actually enhance. With these issues, volume-targeted air flow may be greatest in this patient inhabitants, given the strict control of minute ventilation it permits. Before you get a word out, your attending sees how sick the affected person is, notices your ventilator settings, and questions when you thought-about different, more "complicated" modes of mechanical air flow. The nice majority of patients, whatever the etiology of their respiratory failure, can be managed with typical modes of mechanical ventilation, similar to volume- or pressure-targeted assist control. However, in certain medical conditions, different modes of mechanical air flow may be employed. However, the physiologic rationale does make sense in certain scientific situations. Airway Pressure Release Ventilation Airway strain launch air flow has been described within the literature since 1987. Alveolar recruitment is a pan-inspiratory phenomenon and alveoli which would possibly be recruited are extra compliant than actively recruiting or nonrecruited alveoli. Ventilation is determined by the stored kinetic power at the excessive strain and the intermittent release phase and is augmented by spontaneous breathing. Although minute ventilation is decreased with this mode ventilation, ventilation can additionally be improved by a lower in useless space. Clinical data are restricted however have proven improved oxygenation and fewer shunt and dead house, in addition to decreased want for sedation and neuromuscular blockade. These embrace some convective fuel transport, but additionally molecular diffusion, pendelluft, coaxial circulate, and Taylor dispersion. The bias move delivers contemporary gasoline into the ventilator circuit at forty to 60 L/min, and helps preserve imply airway strain. It is a pressure-targeted breath, time cycled, with square strain waveform and decelerating variable circulate. In this regard, tidal volume is used as a suggestions control, which changes the strain limit (usually breath to breath) as respiratory mechanics change. It maintains the benefit of guaranteed minute air flow, while limiting pressure, and utilizing a decelerating circulate pattern. The ventilator responds to the mechanical output of the affected person and will amplify patient effort with a preset proportional amount of pressure. Pressure is delivered in proportion to the electrical exercise of the diaphragm, which requires the location of an esophageal electrode (similar to nasograstric tube placement). The ventilator is triggered based mostly on Edi, therefore bettering synchrony, because the time delay from patient effort to breath may be very transient. In patients just lately intubated (< forty eight hours), severely hypoxemic, or hemodynamically unstable, these modes should be prevented. Both modes require an intact ventilator drive, and ongoing assessments of pulmonary mechanics is a necessity. If sudden modifications in respiratory system mechanics occur, the % assist should be adjusted. Your attending concedes that medical data appear to be stronger in your present strategy than for the above more complex modes of mechanical ventilation. You finish rounds pleased that the patient appears to have stabilized for the second and go home wondering tips on how to condense all of the medical situations and sophisticated physiology that just occurred. Understanding the equation of motion will shed gentle on what a ventilator is controlling or focusing on for a given breath.