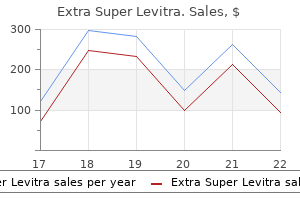
100 mg extra super levitra generic visa
It is advantageous to permit the affected person to sit or to stand by the side of the bed by the evening erectile dysfunction pump extra super levitra 100 mg buy generic on-line. First postoperative day General care: the affected person is predicted to look better and recent impotence in women buy cheap extra super levitra 100 mg. The affected person is inspired to stand or to walk few steps by the facet of the mattress and to sit on the bedside or on a chair. Diet: Oral feeding within the type of plain or electrolyte water is given in small but frequent intervals. With the appearance of bowel sounds or passage of flatus, full liquid food regimen is prescribed. Pain control: Adequate pain control ensures deep breathing, adequate oxygenation, early mobilization, immediate wound healing, lowered pulmonary complication and fewer hospital stay. For this objective, intramuscular injection of pethidine hydrochloride 100 mg or morphine sulfate 10 mg is run at an interval of 6�8 hours. Patient is instructed to use a preset dose (1 mg) of morphine with none overdosage. Antibiotics: Perioperative prophylactic antibiotics as talked about in preoperative care are to be thought-about. This must be administered parenterally for forty eight hours followed by oral route for one more 3 days. Following removal of catheter, postoperative urinary retention is a standard downside. This is as a outcome of of ache, spasm of the pelvic ground muscular tissues, tissues edema or following regional anesthesia. Residual urine is measured after micturition with ultrasound scan or by a catheter. Mobilization: the affected person ought to be inspired to move freely in mattress and to lie in any posture comfortable to her. Deep breathing and movements of the legs and arms are inspired to decrease Third and fourth postoperative days Daily remark of significant indicators twice daily is to be done as a routine. The bowels normally move usually, in any other case low enema or suppository could additionally be given. Fifth and sixth postoperative days the stomach stitches are normally removed on the fifth day in transverse incision and on sixth day in vertical incision. The stitches are to be eliminated in early morning with the affected person in empty abdomen. The precaution is taken, in order that emergency restore of the wound can be accomplished, if burst abdomen happens. Local ache and edema may be relieved by hot compress with magnesium sulfate or infrared rays. While an uniform guideline is tough to formulate, in an in any other case uneventful postoperative restoration, the affected person could also be discharged by 5�7 days following hysterectomy. Examination Prior to discharge Abdominal operation Abdominal wound is to be thoroughly checked for evidences of sepsis, hematoma or dehiscence. If the discharge is offensive, gentle vaginal exploration by a finger must be carried out to exclude a foreign physique (gauze piece). Vaginal exploration with a finger is helpful to detect by accident a retained and forgotten gauze piece. Such operations are widespread and some may need to do it following graduation during home officer job. While in some cases, dilatation of the external os is enough but in majority, the complete canal together with the inner os is to be dilated. When the inner os is to be dilated, prior introduction of uterine sound is mandatory to confirm the position of the uterus. The operation is completed underneath basic anesthesia or underneath diazepam sedation with or with out paracervical block. Such issues are: Injury to the cervix Uterine perforation Injury to the intestine Infection. Injury to the cervix: the injury to the lip of cervix is attributable to vulsellum chew or lateral tear by dilator. The bleeding from the vulsellum site is normally slight and stopped by gauze strain or at greatest by a hemostatic suture. Management of lateral tear: If slight, hemostasis is efficient by intracervical or vaginal gauze plugging. The brisk hemorrhage is probably going due to injury of the descending cervical artery and requires hemostatic sutures taking deep chew of the cervical tissue on the identical side. If however, the tear extends upwards to involve the uterine artery, laparotomy has to be accomplished together with resuscitative measures. Hemostasis is achieved by opening the anterior leaf of the broad ligament failing which ligation of the anterior division of the interior iliac artery may have to be done, if the uterus is to be preserved. Uterine perforation: Uterus is perforated by uterine sound, or dilator or uterine curette. Management: Attempt to verify the perforation by reintroducing the instrument is to be condemned. Once perforation is suspected, following tips are to be followed: To cease the operative process. An uterine sound is launched to affirm the position and to note the size of the uterocervical canal. Hawkin-Ambler dilator should be held in such a means that the knob is contained in the palm and the index finger rests on the body of the instrument. The tip of the finger should be placed at a distance of about 3 cm (slightly greater than the length of the cervical canal) from the tip of the instrument. The tip of the dilator must be directed anteriorly or posteriorly according to the place of the uterus. When the dilator is introduced, the cervix is made steady by traction of the vulsellum. After the desired dilatation, the uterine cavity is curetted by an uterine curette either in clockwise or anticlockwise path ranging from the fundus down to internal os. In benign lesion, sharp curette and in suspected malignancy, blunt curette is used. Vigorous curettage might harm the basal layer of the endometrium and uterine muscle. The curetted material is preserved in 10 % formol-saline (normal saline in suspected tubercular endometritis), labeled properly and sent for histological examination. Usually the perforation is massive and related to varying levels of inside hemorrhage. Associated gut injury is to be appeared for and if discovered, to be tackled accordingly - repair or resection. If laparoscopy facilities can be found, it can be employed in all cases at the earliest.
Aloe perfoliata (Aloe). Extra Super Levitra.
- How does Aloe work?
- Psoriasis.
- Are there any interactions with medications?
- Dosing considerations for Aloe.
- Wound healing, healing skin sores, frostbite, burns, genital herpes, high cholesterol, skin problems caused by radiation used to treat cancer, arthritis, fever, ulcerative colitis, itching, stomach ulcers, diabetes, and asthma.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96602
Extra super levitra 100 mg order amex
If Na+ consumption exceeds Na+ excretion (positive Na+ balance) erectile dysfunction quality of life discount extra super levitra 100 mg amex, then an increase in blood volume will trigger a proportional improve in urinary Na+ excretion impotence young adults 100 mg extra super levitra with amex. The renin-angiotensin-aldosterone system is the bestunderstood hormonal system modulating renal Na+ excretion. This phenomenon, called aldosterone escape, is defined by decreased proximal tubular Na+ reabsorption following blood quantity growth. Harris the scale of a kidney and the whole number of nephrons formed late in embryologic improvement depend on the diploma to which the ureteric bud undergoes branching morphogenesis. Humans have between 225,000 and 900,000 nephrons in every kidney, a quantity that mathematically hinges on whether or not ureteric branching goes to completion or is terminated prematurely by one or two cycles. Although the signaling mechanisms regulating cycle quantity are incompletely understood, these last rounds of branching likely determine how properly the kidney will adapt to the physiologic demands of blood strain and physique measurement, varied environmental stresses, or unwanted irritation resulting in continual renal failure. One of the intriguing generalities regarding persistent renal failure is that residual nephrons hyperfunction to compensate for the lack of those nephrons succumbing to primary illness. This compensation is dependent upon adaptive modifications produced by renal hypertrophy and changes in tubuloglomerular suggestions and glomerulotubular steadiness, as advanced within the intact nephron hypothesis by Neal Bricker in 1969. These three necessary notions regarding chronic renal failure type a conceptual foundation for understanding common pathophysiology leading to uremia. Neilson frequent mechanisms of pRogRessiVe Renal disease When the initial complement of nephrons is lowered by a sentinel occasion, corresponding to unilateral nephrectomy, the remaining kidney adapts by enlarging and growing its glomerular filtration rate. If the kidneys were initially regular, the filtration price often returns to 80% of normal for 2 kidneys. The remaining kidney grows by compensatory renal hypertrophy with little or no cellular proliferation. This distinctive occasion is achieved by growing the dimensions of every cell along the nephron, which is accommodated by the elasticity or progress of interstitial areas under the renal capsule. Hyperfiltration during being pregnant or in humans born with one kidney or who lose one to trauma or transplantation typically produces no sick consequences. This maladaptive response is referred to clinically as renal development, and the pathologic correlate of renal progression is the relentless advance of tubular atrophy and tissue fibrosis. The mechanism for this maladaptive response is the focus of intense investigation. A unified concept of renal progression is just beginning to emerge, and most significantly, this progression follows a ultimate common pathway no matter whether or not renal harm begins in glomeruli or within the tubulointerstitium. Although varied forms of renal harm have their own unique charges of progression, one of the best understood is that related to type I diabetic nephropathy. Notice the early increase in glomerular filtration rate, followed by inexorable decline associated with rising proteinuria. Significant ablation of renal mass leads to hyperfiltration characterised by an increase within the price of singlenephron glomerular filtration. The remaining nephrons lose their ability to autoregulate, and systemic hypertension is transmitted to the glomerulus. Both the hyperfiltration and intraglomerular hypertension stimulate the eventual appearance of glomerulosclerosis. On occasion, inflammation that begins within the renal interstitium disables tubular reclamation of filtered protein, producing gentle nonselective proteinuria. Renal irritation that initially damages glomerular capillaries usually spreads to the tubulointerstitium in affiliation with heavier proteinuria. Many scientific observations help the affiliation of worsening glomerular proteinuria with renal development. The simplest clarification for this enlargement of mononuclear cells is that increasingly extreme proteinuria triggers a downstream inflammatory cascade in tubular epithelial cells, producing interstitial nephritis, fibrosis, and tubular atrophy. Furthermore, glomerular injury either provides activated mediators to the proteinuric filtrate or alters the steadiness of cytokine inhibitors and activators such that attainment of a crucial degree of activated cytokines eventually damages downstream tubular nephrons. The immunologic mechanisms for spreading embrace loss of tolerance to parenchymal self, immune deposits that share cross-reactive epitopes in either compartment, or glomerular harm that reveals a brand new interstitial epitope. The basic mechanisms of renal progression advance sequentially via six phases that include hyperfiltration, proteinuria, cytokine bath, mononuclear cell infiltration, epithelial-mesenchymal transition, and fibrosis. Some experimental interstitial lesions are histologically analogous to a cutaneous delayed-type hypersensitivity reaction, and extra intense reactions generally induce granuloma formation. The cytotoxic activity of antigen-reactive T cells most likely accounts for tubular cell destruction and atrophy. Cytotoxic T cells synthesize proteins with serine esterase exercise in addition to pore-forming proteins, which may effect membrane injury very like the activated membrane attack complex of the complement cascade. Persistent cytokine exercise throughout renal irritation and disruption of underlying basement membranes by native proteases initiates the process of transition. Rather than collapsing in to the tubular lumens and dying, some epithelia become fibroblasts while translocating back in to the interstitial space behind deteriorating tubules via holes in the ruptured basement membrane; the contribution of endothelial cells from interstitial vessels may be equally important. Fibroblasts that deposit collagen during fibrogenesis also replicate regionally at sites of persistent inflammation. Estimates point out that greater than half of the whole fibroblasts found in fibrotic renal tissues are products of the proliferation of newly transitioned or preexisting fibroblasts. After fibroblasts purchase an artificial phenotype, expand their inhabitants, and regionally migrate round areas of irritation, they start to deposit fibronectin, which supplies a scaffold for interstitial collagens. When fibroblasts outdistance their survival elements, they die from apoptosis, leaving an acellular scar. This transport perform and its contribution to sustaining extracellular blood volume often remains near normal till limitations from advanced renal disease inadequately excrete dietary Na+ consumption. Prior to this level and all through renal progression, rising the fractional excretion of Na+ in ultimate urine at progressively lowered rates of glomerular filtration provides a mechanism of early adaptation. Na+ excretion increases predominantly by reducing Na+ reabsorption within the loop of Henle and distal nephron. An increase in the osmotic obligation of residual nephrons increases tubular water and lowers the concentration of Na+ in tubular fluid, decreasing environment friendly Na+ reclamation; increased excretion of inorganic and natural anions also obligates more Na+ excretion. In addition, hormonal influences, notably elevated expression of atrial natriuretic peptides that improve distal Na+ excretion, play an essential function in maintaining internet Na+ excretion. Eventually, with advancing nephron loss, the atrial natriuretic peptides lose their effectiveness, and Na+ retention results in intravascular volume enlargement, edema, and worsening hypertension. Persistent intraglomerular hypertension is associated with progressive nephron destruction. The vasoconstrictive agent endothelin has also been implicated in hyperfiltration, and increases in afferent vasodilatation have been attributed, no much less than partially, to native prostaglandins and release of endotheliumderived nitric oxide. This suggestions originates from the macula densa and modulates renal blood flow and glomerular filtration (see Chap. Glomerulotubular stability outcomes both from tubular hypertrophy and from regulatory adjustments in tubular oncotic stress or solute transport along the proximal tubule. Some research indicate these alterations in tubule dimension and performance may themselves be maladaptive, and as a trade-off, predispose to further tubule harm.
100 mg extra super levitra order with visa
When mixed with stress incontinence impotence type 1 diabetes extra super levitra 100 mg on-line, unstable bladder is to be treated first earlier than proceeding to surgical correction for stress incontinence impotence young men extra super levitra 100 mg overnight delivery. Failed surgical remedy of stress incontinence is to be evaluated for the presence of unstable bladder. In bladder drill, the affected person is instructed to void by the clock at progressively rising intervals over a 6-week time interval. The drill is, however, not useful the place neurologic illness is liable for unstable bladder. Drug remedy: Aims are to-(i) Inhibit bladder contractility, (ii) Increase bladder neck and urethral resistance. The different drugs used are: Trospium chloride (atropine by-product with antimuscarinic effects) and Propiverine (anticholinergic and calcium channel blocker). In addition, the peri or postmenopausal girls are sometimes helped by estrogen therapy. It ought to be remembered that the entity is simply too often associated with real stress incontinence (Table 24. One has to search for perineal sensation, pelvic muscle tone and bulbocavernous reflex to know the integrity of the sacral reflex S2-4 (gentle clitoral stroke ought to produce anal sphincter contraction). The findings are normal or coarse trabeculation and diverticulae of bladder may be seen. This happens in a stable bladder and with none anatomic descent of urethra and bladder neck. However, in many ladies (50�60%), urge symptoms are improved after midurethral sling process (p. Other agents used are: Resiniferatoxin is stronger than Capsaicin and less unwanted aspect effects of pain and burning). Botulinum toxin is a neurotoxin discovered to efficient in intractable detrusor over exercise. Surgery: In intractable instances not relieved by drugs or bladder irritability because of neurologic disease, surgical procedure could additionally be of help. This is within the form of denervation ( to interrupt the nervous pathways), augmentation cystoplasty ( to increase bladder capacity) or urinary diversion (ideal conduit). Overactive bladder (OaB) leakage of urine because of detrusor over activity during the filling section while the affected person tries to inhibit it. Diminished bladder capacity normal cystourethroscopy lateral cystourethrography offending issue present (Table 24. Therefore urgency and ache are the two important diagnostic standards of painful bladder syndrome. The probable causes are: allergic, autoimmune, infective, toxins or leaky urothelium secondary to poor glycosaminoglycan layer. Symptoms include urgency, frequency, pelvic and lower urinary tract pain, dyspareunia and urinary incontinence. On distension, petechial hemorrhages with oozing of blood from the surface is commonly seen. Behavioral therapy, pelvic flooring bodily therapy, medicines together with hormones and bladder instillation are the therapy options. Drugs: Urinary tract analgesics like hyoscyamine, phenyl salicylate might scale back urethral irritation. Glomerulations (petechial hemorrhages) could additionally be seen in the bladder mucosa after hydrodistension. Its mechanism might be the over-distension of the bladder pulls open the internal sphincter. The causes of overflow incontinence are the same as retention of urine which will be mentioned later in the chapter. Cystometry reveals giant capacity of the bladder and no rise of detrusor pressure during voiding. Normally for complete emptying of bladder, pelvic ground muscle (levator ani) and urethral sphincter (intrinsic rhabdosphincter) should chill out and on the similar time the detrusor must contract. Voiding difficulties could lead to retention of urine either acute (inability to void more than 12 hours without catheterisation) or chronic (inability to empty the bladder greater than 50 percent of its volume). The components working are: � Obstructive due to postoperative edema within the neighborhood of the sew line. Following radical operation: � Denervation of the nerve supply of the bladder which travels from S2,three,four in the parametrium. Obstructive circumstances intrinsic to the urethra A pelvic tumor or a mass in the pelvis might produce retention of urine. Retention is attributable to the tumor interfering with the opening of inner sphincter of the urethra. Spasm of external sphincter acute retention: Catheterization is to be carried out by utilizing an autoclaved gentle rubber catheter. If the affected person fails to cross urine normally once more after 8 hours, a self-retaining catheter is to be launched for continuous drainage for at least 24�48 hours. Under no circumstances, the residual urine should exceed one hundred mL, preferably under 50 ml. Moreover, in circumstances of asymptomatic bacteriuria, the infection remains within the urinary tract for a long time frame only to flare up to produce pyelonephritis in important instances. As such, due consideration ought to be paid even in asymptomatic sufferers having vital bacteriuria. Sexual intercourse increases the ascent of the organisms from the lower urethra in to the bladder. But certain circumstances favor atonicity of the bladder and urinary stasis as in being pregnant, puerperium and following major pelvic surgical procedure or pelvic tumors producing outflow tract obstruction. Catheterization-This might be the most typical reason for introducing the organisms from the decrease urethra in to the bladder no matter meticulous aseptic technique being taken. It has been noticed that an indwelling catheter kept for 24 hours will produce bacteriuria in 50 percent and if left for four days will result in bacteriuria in 100 percent of circumstances. Hypoestrogenic state as in postmenopausal women-when defence of the bladder and urethral mucosa is diminished. Close proximity of the external urethral meatus to the areas (vulva and lower-third of vagina) contaminated closely with micro organism. The organisms from the anorectal region, lower vagina and vulva gain entry to the urethra and thence to the bladder and kidneys. Hematogenous-spread involving the kidneys is from the gut or septic tonsils or different septic foci. Lymphatic-spread is either from the adjoining ascending colon or genital organs (cervicitis).
Generic 100 mg extra super levitra with mastercard
Women and those with darker pores and skin may be extra more likely to erectile dysfunction doctor dallas extra super levitra 100 mg generic amex current to medical attention disease that causes erectile dysfunction purchase 100 mg extra super levitra amex. Most affected people develop lesions earlier than 20 years of age and experience a progressive enhance in depigmentation over time. Affected pores and skin may be extra vulnerable to cell loss by way of apoptosis and via melanocytorrhagy, which is the upward migration and lack of melanocytes through the stratum corneum due to insufficient cell adhesion. Genetically mediated illness susceptibility underlies each of the above mechanisms of melanocyte cell loss. Clinical Presentation History Initial onset could additionally be sudden, however the affected person will normally report gradual, progressive enlargement of white spots on the pores and skin with out related signs. A personal history of autoimmune disease or household historical past of vitiligo may be present. Sun exposure or trauma could draw consideration to the lesions, causing the patient to seek medical consideration. Subjectively, the patient could express emotional distress over the conspicuous and disfiguring lesions. Laboratory Findings No abnormalities are seen in routine laboratory studies; nevertheless, patients may have evidence of thyroid abnormalities or different autoimmune diseases. Histologically, vitiligo is characterised by the absence of melanocytes in affected pores and skin, though degenerating melanocytes may be seen in lesional borders. Conversely, regular melanocytes are seen in clinically nonaffected skin, but keratinocytes could seem abnormal, with extracellular granular material and vacuolated cytoplasm within the basal layer. Physical Examination Stark white, well-demarcated macules of various sizes are famous in 5 attainable patterns. Lesions are sometimes symmetric but may happen anyplace with a peculiar predilection for circumferential involvement of orifices, face and higher chest, and sites of stress. Vitiligo on knees in a patient after ultraviolet gentle therapy, note small areas of repigmentation of pores and skin with treatment. Pityriasis alba: A comparatively common condition in kids with atopy; also may have fantastic scale, however lesions retain some pigment and are less sharply demarcated. Postinflammatory hypopigmentation: A historical past of trauma or inflammation of the affected space will precede the lack of pigment. Guttate hypomelanosis: Presents with hypopigmented macules in a photodistribution on a background of actinic harm primarily on the legs and arms; not like vitiligo, the macules are often 5 mm in diameter or less. Chemical leukoderma: Certain chemical compounds, notably aromatic derivatives of phenols and catechols, can destroy melanocytes, leading to chemical leukoderma that might be differentiated from vitiligo by the historical past of toxin exposure, lesions with weird borders and scale, a "confetti-like" distribution, and symptomatic pruritus. Ash leaf spots of tuberous sclerosis: Accompanied by angiofibromas, periungual fibromas, connective tissue nevi, and presumably neurological sequelae. Management the speed of spontaneous repigmentation is as high as 20%,1 however is usually incomplete. Treatment is almost at all times undertaken because of the often progressive course and important psychosocial burden of illness. A multifaceted strategy is used primarily based on the varied mechanisms contributing to vitiligo. Immunosuppression quiets the autoimmune contribution and stimulation of melanin production counteracts the progressive lack of melanocytes. Topical corticosteroids, calcineurin inhibitors (pimecrolimus cream, tacrolimus ointment), and vitamin D3 supplementation could improve vitiligo by affecting the immune system regionally. Light remedy generally causes itching, dry pores and skin, and generally perilesional hyperpigmentation. Oral antioxidants such as nutritional vitamins C and E could also be helpful adjuncts to minimize oxidative injury from free radicals current in lesional pores and skin. Finally, a number of surgical strategies for autologous transplantation (such as punch-grafting, split-thickness grafting, and epidermal blister grafts) have been employed with good to excellent success in patients resistant to other medical therapies. Donor website cells could even be cultured to allow remedy of extra extensively affected regions. Again, a mix of medical and surgical remedy is commonly used to maximize repigmentation. Aside from influencing disease exercise, specialized makeup could also be surprisingly effective in evening pores and skin tone. The reverse strategy is sometimes taken for extensive illness involving greater than 50% of the physique surface space by depigmenting regular skin to attain the aim of homogenous skin coloration. In addition to vigilant sunscreen use, meticulous search for skin cancers is required, as the depigmented pores and skin is vulnerable to the deleterious results of sun harm. Concomitant autoimmune problems should be sought with thyroid studies, screening for antinuclear and different organ-specific antibodies, and hematologic analysis. Information on assist teams ought to be offered to sufferers with vitiligo because of the potential for vital psychosocial effects and negative impression on quality of life associated with this condition. In addition, vitiligo sufferers undergo an increased rate of psychiatric comorbidity, and when needed, acceptable psychiatric referral should be given. The National Vitiligo Foundation provides instructional materials, reviews clinical trials and research updates, and help teams on the website: The onset of melasma following pregnancy or use of oral contraceptives implicates hormones as a precipitating issue, presumably via upregulation of the estrogen receptor and its diversified downstream results. Most doubtless, multiple mechanisms act synergistically to induce disease in genetically prone individuals. Medications: Such as minocycline, could cause facial pigmentation, but is often current in sun-protected areas as well and one typically elicits a historical past of drug ingestion with the onset of the pigmentation. Management the targets of melasma remedy are to forestall new pigment manufacturing through each pharmacologic and physical means and to lighten affected pores and skin by reducing melanosomes. Skin irritation is the most typical aspect impact noticed, however nowadays that is often due to the various extra parts in presently available preparations. The most serious facet effect of continual use is ochronosis, which is a pepper-like deposition of hydroquinone in the pores and skin, although this situation is rare in the United States. Topical retinoids have additionally been shown to scale back pigmentation in skin affected Diagnosis the key diagnostic options of melasma are tan to brown macules in the centrofacial areas of girls. Differential Diagnosis Postinflammatory hyperpigmentation: Presents with an antecedent history of trauma or irritation. Solar lentigines: Usually more diffuse, not essentially symmetrical, and related to other evidence of actinic injury, as is actinic lichen planus. Medication Hydroquinone: 2% formulations are over-the counter 4% formulations are prescription solely Examples of Brand Name(s) Aclaro, Alphaquin, Alustra, Claripel, Eldopaque, Eldoquin, EpiQuin Micro, Esoterica, Glyquin, Lustra, Melpaque, Melquin, Nuquin, Solaquin, Melanex, Melanol, Viquin Tri-Luma Dosing Twice day by day to affected areas Notes Side results: pores and skin irritation (particularly when combined with tretinoin and alpha hydroxy acids) and ochronosis (rare) Pregnancy class C Moderate efficacy Side results: Skin irritation, primarily as a outcome of tretinoin Pregnancy class C Most efficacious Side results: Skin irritation and threat of allergy Moderate efficacy Triple mixture cream (Fluocinolone acetonide 0. Improvement is usually seen in 1 month however could take as a lot as 6 months for max effect. Published stories of huge series of patients on day by day hydroquinone have shown that it could possibly safely be used for no less than 1 year. Chemical peels could additionally be of modest profit as an adjunct in recalcitrant illness, but with the danger of exchanging melasma for postinflammatory hyperpigmentation. Preliminary research with laser and light remedies are promising, however additional studies are required to higher outline their dangers, benefits, and function within the remedy of melasma.
Cheap 100 mg extra super levitra amex
Premature menarche the other causes of vaginal bleeding erectile dysfunction vitamin e 100 mg extra super levitra cheap with amex, corresponding to overseas body or harm has to be excluded erectile dysfunction causes and cures cheap extra super levitra 100 mg otc. It must be borne in mind that even in instances when no trigger can be detected in any of the types talked about, the periodic evaluation at 6 month-to-month intervals is to be made to detect any life-threatening pathology at the earliest. The exogenous estrogen remedy or its inadvertent intake should be stopped forthwith. Cortisone remedy for adrenal hyperplasia and surgical procedure to take away the adrenal or ovarian tumor remove the surplus supply of both androgen or estrogen. To suppress gonadal steroidogenesis or counteract the peripheral action of sex steroids. The agonists suppress the untimely activation of hypothalamopituitary axis due to down regulation and thereby diminished estrogen secretion. Cyproterone acetate-It acts as a potent progestogen, having agonist effects on progesterone receptors. Overall prognosis is nice with main hypothyroidism, adrenal or ovarian tumors following therapy. Apart from the brief stature due to accelerated bone fifty four TexTbook of GynecoloGy Eventually the vast majority of these teenaged girls establish a traditional cycle and are fertile. Anovulatory cycles unopposed estrogen endometrial hyperplasia extended and heavy intervals (see p. Evaluation is very indicated if the menstrual interval is < 22 days or > forty four days, lasts longer than one week or the bleeding is too heavy that anemia develops. Investigations include, routine hematological examination, together with bleeding time, clotting time, platelet rely. Management: the girl wants adequate rationalization, reassurance and psychological help. In refractory instances, proge- maturation, the idiopathic group have gotten a traditional menstrual sample in future. Assurance, enchancment of basic health and therapy of any illness could also be of help in nonendocrinal causes. Cases of hypergonadotropic hypogonadism should have chromosomal research to exclude intersexuality (see p. The condition often turns into normal following 2�3 programs after which normal cycles resume. Regular menstrual cycle shall be established once the hypothalamo-pituitary-ovarian axis is matured. The most typical order of adjustments is starting of progress spurt Enlargement of the breast buds Appearance of pubic hair Axillary hair Peak progress in peak Menstruation (menarche). The time period precocious puberty is reserved to those that exhibit any secondary sex characteristic before the age of eight or menstruate before the age of 10. The main purpose of management for a girl with precocious puberty is to (i) reduce the secretion of gonadotropins. The different drugs used for constitutional kind to suppress the premature activation of hypothalamo-pituitary� gonadal axis are-medroxyprogesterone acetate, cyproterone acetate, and danazol. Ovarian failure and chromosomal anomalies are the frequent causes of delayed puberty. Estimation of serum gonadotropins is essential to differentiate hypogonadotropic from hypergonadotropic causes (Table 5. Menstruation just after puberty and just before menopause are largely anovulatory and sometimes irregular in frequency. Pubertal menorrhagia must be handled with rest, assurance, hematinics and blood transfusions. The medical analysis is confirmed following stoppage of menstruation (amenorrhea) for twelve consecutive months with out any other pathology. Premenopause refers to the period prior to menopause, postmenopause to the interval after menopause and perimenopause to the period around menopause (40�55 years). Climacteric is the time period throughout which a woman passes from the reproductive to the nonreproductive stage. Perimenopause is the part of the climacteric when the menstrual cycle is prone to be irregular. It can be not associated to number of pregnancy, lactation, use of oral tablet, socioeconomic situation, race, peak or weight. As a outcome, efficient folliculogenesis is impaired with diminished estradiol production. There is a major fall within the degree of serum estradiol from 50�300 pg/mL earlier than menopause to 10�20 pg/mL after menopause. Disturbed folliculogenesis throughout this period may result in anovulation, oligo-ovulation, untimely corpus luteum or corpus luteal insufficiency. The sustained degree of estrogens might even trigger endometrial hyperplasia and medical manifestation of menstrual abnormalities prior to menopause. The muscle coat becomes thinner, the cilia disappear and the plicae turn into much less distinguished. The uterus becomes smaller and the ratio between the physique and the cervix reverts to the 1:1 ratio. In some women, however, with high endogenous estrogens, the endometrium could also be proliferative and even hyperplastic. Loss of muscle tone leads to pelvic leisure, uterine descent and anatomic modifications in the urethra and neck of the bladder. The pelvic mobile tissues turn out to be scanty and the ligaments supporting the uterus and vagina lose their tone. Estradiol production drops right down to the optimal level of 20 pg/mL no endometrial development absence of menstruation. Estrogens Following menopause, the predominant estrogen is estrone and to a lesser extent estradiol. Serum level of estrone (30�70 pg/mL) is higher than that of estradiol (10�20 pg/mL). The major supply of estrone is peripheral conversion (aromatization) of androgens from adrenals (mainly) and ovaries. The trace amount of estradiol is derived from peripheral conversion of estrone and androgens. Though the secretion of androgens from postmenopausal ovary are extra, their peripheral levels are reduced as a outcome of conversion of androgens to estrone in adipose tissue. Progesterone: A trace amount of progesterone detected is probably adrenal in origin. Estrogen will increase absorption of calcium from the gut, stimulates calcitonin secretion from the C cells of the thyroid and will increase 1, 25 dihydroxy vitamin D. The essential symptoms and the health concerns of menopause are: Vasomotor symptoms Urogenital atrophy Osteoporosis and fracture Cardiovascular disease Cerebrovascular disease Psychological adjustments Skin and Hair Sexual dysfunction Dementia and cognitive decline.
Generic extra super levitra 100 mg without prescription
It is due to no xplode impotence extra super levitra 100 mg cheap line high sodium chloride and low protein content material in the mucus as a outcome of common causes erectile dysfunction extra super levitra 100 mg buy discount line excessive estrogen within the midmenstrual section prior to ovulation. After ovulation with rising progesterone, the ferning disappears completely after twenty first day. Thus, the presence of ferning even after twenty first day suggests anovulation and its disappearance is presumptive evidence of ovulation. The cervical scoring system of Insler (1979) takes in to the account the quantity, spinnbarkeit, ferning of the mucus along with state of the external os of the cervix. Principle: It is the examination of the cervical mucus to evaluate the presence of progressively motile sperm in it. Presence of no less than 10 progressively motile sperm per excessive energy subject signifies the check is regular. Colposcope and colpomicroscope are the low-power binocular microscope, mounted on a stand. It is designed to magnify the surface epithelium of the vaginal a part of the cervix including whole transformation zone. The magnification is to the extent of 15�40 occasions in colposcopy and about 100�300 instances in colpomicroscopy. Colposcopic examination of the cervix and vagina is completed utilizing low power magnification (6-16 fold). Cervix is then cleared of any mucus discharge using a swab soaked with normal saline. Next, the cervix is wiped gently with three p.c acetic acid and examination repeated. Higher is the frequency of ultrasound wave, higher is the image decision however lesser is the depth of tissue penetration. This flow can be measured by analysis of the waveform utilizing the pulsatility index. The favorable periovulatory endometrium ought to be between 7 and 11 mm thick (see Chapter 16) Ultrasound can provide presumptive proof of ovulation. Following ovulation, internal echoes seem inside ruptured follicle and free fluid is noticed in pouch of Douglas To detect right timing of ovulation by folliculometry along side plasma estradiol. Low circulate impedance with excessive flow velocity raises the suspicion of a malignant tumor. Presence of papillary excrescences, mural nodules, septations, cystic lesion with stable components, snow storm appearance (hydatidiform mole) and ascites are the opposite sonographic features of malignancy. Endometrial biopsy is required for postmenopausal ladies with thicker endometrium (see p. This technique could be utilized for many diagnostic and therapeutic functions: Aspiration of cystic plenty. In obese or in instances of distended stomach or gut, it is an ideal alternative to sonar. Normal saline is infused slowly (5�10 mL) when the uterus is imaged with vaginal ultrasound. Cross-sectional photographs of the physique are taken at very shut intervals (few millimeters thick) within the form of a number of slices. When a pulse of radiowaves is imposed on the nuclei a strong resonance will happen and the energy is absorbed by the nuclei. Hence, caution should be exercised with epileptic sufferers and who had recent myocardial infarction. Cancer tissues process this glucose analogue in another way in comparison with that of regular tissues. Ultrasound guided procedures are used for each the diagnostic and therapeutic purposes. It may be employed in chosen circumstances to detect microadenoma of pituitary or metastatic lesions in the brain or liver. Biopsy may be taken safely on the outpatient division, if the pathology is detectable, however for wider tissue excision as in cone biopsy, it should be accomplished as an inpatient procedure. A skinny plastic cannula (2�4 mm diameter), with a plunger within, is negotiated within the uterus. When the plunger is withdrawn, sufficient endometrium is obtained due to suction motion. Indications of endometrial sampling are: (a) Dysfunctional uterine bleeding; (b) Abnormal bleeding following the utilization of hormone substitute remedy; (c) Abnormal perimenopausal or menopausal bleeding. To examine the hormonal effect, material from the fundus and upper part of the physique is to be taken. However, additional diagnostic procedures, corresponding to hysteroscopy should be accomplished when needed. When a large tissue mass is needed for histological studies, a thorough endometrial curettage is to be accomplished beneath anesthesia as in endometrial tuberculosis or postmenopausal bleeding. Indications In suspected disturbed ectopic pregnancy or different causes producing hemoperitoneum In suspected cases of pelvic abscess. The procedure is completed beneath sedation the patient is put in lithotomy position Vagina is cleaned with Betadine A posterior vaginal speculum is inserted An 18 gauge spinal needle fitted with a syringe is inserted at a degree 1 cm beneath the cervicovaginal junction within the posterior fornix. If unclotted blood is obtained, the prognosis of intraperitoneal bleeding is established. If no blood or fluid is obtained, the needle is withdrawn slowly whereas intermittent suction should be maintained. Follow-up of pelvic surgery (second look) � Tuboplasty � Ovarian malignancy � Evaluation of therapy in endometriosis. Its use is gradually widening both in diagnostic and therapeutic field in gynecology. Timing of laparoscopy: In infertility work up, it could be accomplished in the periovulatory interval to facilitate chromopertubation and likewise prognosis of ovulation. The instrument is to pass transcervically, normally without dilatation of the cervix or local anesthesia. However, for operative hysteroscopy, both paracervical block or common anesthesia is required. Diagnostic hysteroscopy should be performed within the postmenstrual period for better view with out bleeding. The interpretation of endometrial pathology is similar to colposcopy in that it depends on shade, contour and vascular sample. Indications: Diagnostic Operative the technical details and operative hysteroscopy are dealt in Chapter 35. Diagnostic Unresponsive irregular uterine bleeding to exclude Conclusion: the devices for endoscopic procedures are pricey and require a substantial quantity of expertise for diagnostic and especially for operative procedures. It should be done routinely in all circumstances of uterine malignancy for clinical staging. It is extended freely to look at virgins or in cases with pediatric gynecological issues. Common hazards are: A -(i) Eyes-visual loss due to corneal or retinal injury, (ii) Skin injury, and (iii) Damage from laser smoke. B -General: (i) Burn harm (use of spirit and paper drapes must be averted in theatre), (ii) Inflammable anesthetic gases are to be used with nice care, (iii) Reflections of laser beam is harmful.
Syndromes
- Remove tampons before inserting the condom.
- Nausea and vomiting
- Infant-only rear-facing seats
- Schizophrenia
- Alcohol abuse
- C-reactive protein
- Radial nerve dysfunction
- Use reminders, notes, lists of routine tasks, or directions for daily activities.
- You have new symptoms, such as fever or pain and redness of the skull behind the ear
- To repair this defect, a cut is usually made on the left side of the chest, between the ribs. There are many ways to repair coarctation of the aorta.
Buy 100 mg extra super levitra otc
The subglottis stretches from 1 cm below the glottis to the lower border of the cricoid erectile dysfunction causes depression 100 mg extra super levitra purchase overnight delivery. In addition webmd erectile dysfunction treatment buy generic extra super levitra 100 mg on line, during swallowing, the larynx is elevated pari passu with the hyoid bone so as to relaxation underneath the tongue. Nerve provide the pharynx is provided by nerve branches from the pharyngeal plexus. Taste to the anterior two-thirds of the tongue is via the chorda tympani nerve which runs in the lingual nerve and through the glossopharyngeal nerve for the posterior one-third and the pharyngeal wall. The high quality of the raw fundamental laryngeal phonatory sound is further altered by the resonating cavities of the pharynx, mouth and nose. The functions of the salivary glands are related to the properties and volume of saliva (Table three. Lymphatic drainage Lymph nodes within the head and neck provide a barrier to the spread of illness, either inflammatory or neoplastic. Enlargement both implies main disease of the nodes or is secondary to pathology in the head and neck, but much less generally from websites Table 3. Direct questioning associated to particular areas in the throat is important, and smoking habits and alcohol intake should be assessed. Blockage of a duct of the sublingual salivary gland may give rise to a cystic lesion known as a ranula in the floor of the mouth. Intake of alcohol, ingestion of garlic and use of tobacco will also give rise to a foul breath. Deafness could occur because of obstruction of the Eustachian tube with nasopharyngeal pathologies. The alteration in voice in hypopharyngeal neoplasia is due either to direct infiltration of the larynx, by involvement of the recurrent laryngeal nerve with improvement of vocal wire palsy. Secondary nodal neck plenty are very frequent with pharyngeal neoplasia and will be the presenting feature. Maxillary sinusitis might lead to toothache if a tooth root is projecting in to the sinus mucosa. Symptoms, indicators and examination fifty nine Larynx An alteration in voice (dysphonia) is the predominant symptom in laryngeal pathology. Aspiration of solids and liquids could happen with an incompetent larynx because of vocal wire paralysis, but is invariable in neurological disease producing sensory loss of the supraglottis. If related to mastication and a few short-term swelling of the gland, significantly the submandibular, it could be due to an obstructive lesion in the salivary ducts. A permanent enlargement of the salivary gland is neoplastic except proven to the contrary. Contrast swallow studies could provide information on hypopharyngeal and oesophageal pathology. A number of radiological investigations of the salivary glands are available and are chosen in accordance with the suspected pathology (Table 3. A full examination of the higher air and meals passages should be carried out and biopsies taken if malignancy is suspected. Increasingly, laryngopharyngeal examination is carried out utilizing a fibreoptic nasal endoscope. Often, a lesion may be more simply felt than visualized, and its limits readily defined. Symptoms, signs and examination Infective and neoplastic lesions of the upper air and food passages could current as enlarged neck glands. Resolution is spontaneous, although a degree of symptomatic reduction is produced by steam inhalations and voice relaxation. If neoplasia has been excluded, management is directed to avoiding identified aetiological components. Peripheral pathologies embrace myasthenia gravis, motor neurone disease, and lesions affecting the vagus and recurrent laryngeal nerves. Once a vocal twine palsy has been diagnosed and any local laryngeal pathology excluded, a systematic approach is required to determine the aetiology. Because of its longer route, the left recurrent laryngeal nerve is more frequently involved in pathology. On the left this shall be from the skull through the skull base, neck and thorax again to the larynx; on the right it terminates in the neck. Rheumatoid arthritis may find yourself in fixation of the cricoarytenoid joint and vocal cord immobility. Such patients invariably have extreme involvement of the small joints within the arms and toes. This involves techniques to medialize the palsied twine so that the cellular wire is extra simply able to impact approximation. Some recuperate spontaneously (which could take as a lot as 6 months) or turn out to be asymptomatic as the contralateral mobile vocal twine compensates. All cases of continual dysphonia must be referred for laryngeal examination to exclude neoplasia. Avoidance of trauma (tobacco, voice abuse) will hasten decision of acute dysphonia and improve chronic laryngitis. The nodule is located at the junction of the anterior and middle third of the vocal cord. This is the realm of maximum trauma at larger pitch ranges seen in actions similar to screaming and singing. Most instances reveal long-term poor voice high quality of gradual onset, which is mostly worse after a interval of speaking. However, prolonged recurring misuse and abuse of the vocal folds can result in secondary organic modifications. These changes may be reversible by suitable re-education, but in some situations would require surgical intervention. Vocal twine oedema and polyps Oedema of the vocal cords is often symmetrical and impacts the whole length of the twine. Localization of the oedema to a circumscribed web site will produce a polyp, often sited in the anterior third of the vocal wire. The response can generally lead to considerable granulation tissue with the formation of a contact granuloma. Bilateral circumstances without marked granulation may resolve with a combination of voice remedy, antibiotics, antireflux remedy and a lowering course of oral steroids. The cords are reddened, delicate oedema may be present, and submucosal haemorrhages could occur. Treatment is directed at permitting the acute irritation to resolve and correction of underlying poor vocal habits. Retrieval of the voice should be fast, in any other case the risk of the conversion being proof against remedy is high. The voice is characteristically excessive pitched, weak, breathy and monotonous and female in high quality.
Best 100 mg extra super levitra
The caf� au lait spot is a tan to mild brown patch best erectile dysfunction pills for diabetes extra super levitra 100 mg with visa, showing freckle-like usually ranging in measurement from 2 to 20 cm impotence quotes cheap 100 mg extra super levitra mastercard. Laboratory Findings Histopathology of neurofibromas exhibits dermal nerve fibers and spindle cells. Diagnosis To make the diagnosis of neurofibromatosis, two of the next findings have to be current. Pathophysiology Tuberous sclerosis is associated with dysregulation of tumor suppressor function that results in hyperplasia of each ectodermal and mesodermal cell-derived tissues. History and Physical Examination Almost all affected (96%) people may have white or off-white macules, usually referred to as "thumb print" or "ashleaf " macules present at birth or observed within the first 12 months of life. Bilateral optic nerve gliomas Management Management contains observation for growth of associated tumors similar to adrenal pheochromocytoma, sarcomas, optic glioma, acoustic neuroma, and astrocytoma. Connective tissue nevi skin-colored plaques (shagreen patch) Periungual and subungual fibromas Retinal plaques Cardiac rhabdomyomas Central nervous system tumors Seizures B. They also ought to be referred for an ophthalmologic examination and genetic counseling. Once patients are diagnosed, administration often requires a team method with primary care, dermatology, neurology, and different applicable specialists. Diagnosis and Differential Diagnosis For diagnosis see above in clinical presentation. The differential diagnosis for facial angiofibromas includes zits, rosacea, dermal nevi, fibrous papules, and syringomas. Symptomatic cutaneous angiofibromas could be treated with surgical removing and laser. Indications for Consultation Diagnosis and management are often difficult and regularly require a group method with primary care clinicians, dermatology, neurology, geneticists, nephrology, and radiology. The differential analysis for purpura is broad, however it can be quickly narrowed by classifying the lesions based mostly on their morphology, in addition to different medical and laboratory findings. These are often palpable plaques, however can present as nonpalpable patches as nicely (Tables 25-5 and 25-6). When contemplating the differential diagnosis of purpura, it could be very important notice that a few of these A careful history and evaluate of underlying medical circumstances, medicines, and a complete bodily examination can be crucial to the analysis. An optimum biopsy involves appropriate choice of the biopsy type, site, timing, and interpretation of results. Indications for pores and skin biopsy: Palpable and retiform purpura should immediate a pores and skin biopsy. It is necessary to make notice of the age of the lesion, as a illness course of can appear completely different on histopathologic examination at numerous stages. It is important to let the pathologist studying the biopsy understand how lengthy the process has been present. Causes of petechiae (primary lesion is a macule 4 mm) with low platelets (<150,000/L). Causes of petechiae (primary lesion is a macule four mm), with regular to high platelets (>150,000/L). In chilblains, lymphocytic vasculitis with edema and thickening of dermal vessel wall is seen. Retiform purpura without inflammation typically reveals bland thrombi with no inflammation of vessel wall. Purpura on toes with retiform sample on foot in a patient with cholesterol emboli. Usually age <20 years Tetrad: purpura (universal), arthritis (82%), nephritis (40%), abdominal pain (63%), or gastrointestinal hemorrhage (33%) May seem targetoid, on extensor areas and buttock Extension to trunk/upper extremities can indicate renal involvement Persistence of hive-like lesions >24 hours, usually burn > itch. Often multisystemic (eg, constitutional, renal, stomach ache, livedo reticularis, peripheral neuropathies). Causes of retiform purpura, noninflammatory, and related to microocclusive disease. Can have purpura fulminans Branching palpable purpura resulting in peripheral symmetrical gangrene. Causes of retiform purpura, noninflammatory, and associated to microocclusive disease (Continued). Heparin-induced thrombocytopenia: when a low platelet rely is a mandate for anticoagulation. Various causes eg, infection, medications, Henoch Shonlein purpura, blended cryoblobulinemia, rheumatic vasculitis, Wegners, granulomatosis and Churg-Strauss,and so forth. Ahmed Management / 238 References / 242 Pruritus (itch) is the unpleasant sensation of the pores and skin that ends in a need to scratch. Pruritus can vary from mild to extreme, and could additionally be intermittent or chronic (lasting longer than 6 weeks). The International Forum for the Study of Itch printed a scientific classification of pruritus3 by which they proposed 6 classes for pruritus based mostly on the underlying origin: 1. Dermatological: Pruritus related to ailments of the skin, including diseases that function prominent pruritus similar to atopic dermatitis, allergic contact dermatitis, xerotic dermatitis, lichen simplex chronicus, lichen planus, scabies, and urticaria. Systemic: Pruritus associated with ailments in organs aside from the skin, such because the liver, kidneys, hematopoietic system, and so on. Neurological: Pruritus associated with diseases or disorders of the central or peripheral nervous system. Typically, the pruritus in classes 2 to 6 is associated with no main skin lesions. It is necessary to determine the etiology of persistent pruritus, as a outcome of it could be an early symptom of the ailments in categories 2 to four. Table 26-1 incorporates details about chosen illnesses which may be associated with persistent pruritus. Differential analysis of pruritus in sufferers with no underlying skin disease (Continued). Disease Other (of Unknown Origin) Pruritus of the aged Many causes: continual illness, polypharmacy, xerosis, institutionalized care, age-related alterations of skin including atrophy, decreased cutaneous vascular supply, altered lipid composition, altered peripheral nerve innervations, and compromised moisture retention13 Generally secondary to systemic illness or other pores and skin problems There are strict criteria for true idiopathic aquagenic pruritus Etiology unknown Not related to other behaviors or inner abnormalities Resolves with weight restoration15 Generalized or localized Epidemiology/Etiology History and Clinical Presentation of Pruritus Aquagenic pruritus Prickling, stinging, burning, and tingling sensation happen within 30 min of water publicity and lasts as much as 2 h Begins on decrease extremities and generalizes Spares head, palms, soles, and mucosa14 Intermittent or fixed May additionally experience burning or tingling Often localized: neck, thighs, forearms, buttocks, ankles, and higher arm Pruritus in anorexia nervosa Table 26-2. Hyperpigmented, barely lichenified plaque on again brought on by chronic rubbing and scratching. Clinical classification of itch: a position paper for the International Forum for the Study of Itch. Pruritus in being pregnant and childhood-do we actually contemplate all related differential diagnoses Chapter 6 incorporates topical antipruritic medicines and oral medications that could be helpful within the management of patients with pruritus. Other systemic therapies are guided by the underlying reason for pruritus (including anticholestatics, antidepressants, anticonvulsants, thalidomide, and opioid inhibitors). The impression of pruritus on the standard of life of patients present process dialysis: a single centre cohort examine.
Extra super levitra 100 mg discount with amex
It is crucial to appropriate hypernatremia slowly to keep away from cerebral edema impotence yoga poses extra super levitra 100 mg order free shipping, sometimes changing the calculated free-water deficit over forty eight h erectile dysfunction treatment in qatar order extra super levitra 100 mg. Notably, the plasma Na+ focus should be corrected by no extra than 10 mM/d, which may take longer than forty eight h in patients with extreme hypernatremia (>160 mM). Water ideally must be administered by mouth or by nasogastric tube as essentially the most direct method to present free water, i. Depending on the historical past, blood stress, or scientific volume standing, it may be appropriate to deal with initially with hypotonic saline solutions (1/4 or half normal saline); normal saline is usually inappropriate within the absence of very severe hypernatremia, in which normal saline is proportionally more hypotonic relative to plasma, or frank hypotension. For example, decreased distal supply of Na+, as happens in hypovolemic, prerenal states, tends to blunt the flexibility to excrete K+, resulting in hyperkalemia; in distinction, an increase in distal supply of Na+ and distal circulate price, as occurs after treatment with thiazide and loop diuretics, can improve K+ secretion and lead to hypokalemia. Abnormalities within the renin-angiotensinaldosterone system thus may cause both hypokalemia and hyperkalemia. Notably, however, potassium excess and potassium restriction have opposing, aldosteroneindependent effects on the density and exercise of apical K+ channels in the distal nephron; i. Increased 2-adrenergic sympathetic exercise: postmyocardial infarction, head harm three. Increased distal flow and distal Na+ supply: diuretics, osmotic diuresis, salt-wasting nephropathies 2. Distal delivery of nonreabsorbed anions: vomiting, nasogastric suction, proximal renal tubular acidosis, diabetic ketoacidosis, glue sniffing (toluene abuse), penicillin derivatives (penicillin, nafcillin, dicloxacillin, ticarcillin, oxacillin, and carbenicillin) 3. Hypokalemia is related to a tenfold increase in inhospital mortality charges due to opposed results on cardiac rhythm, blood stress, and cardiovascular morbidity price. Systemic hypomagnesemia also can trigger treatment-resistant hypokalemia as a outcome of a combination of decreased mobile uptake of K+ and exaggerated renal secretion. Spurious hypokalemia or pseudohypokalemia occasionally can result from in vitro cellular uptake of K+ after venipuncture, for instance, due to profound leukocytosis in acute leukemia. Inhibition of passive efflux of K+ can also cause hypokalemia, albeit rarely; this usually happens within the setting of systemic inhibition of K+ channels by toxic barium ions. Exogenous insulin could cause iatrogenic hypokalemia, significantly through the management of K+-deficient states such as diabetic ketoacidosis. Alterations within the exercise of the endogenous sympathetic nervous system can cause hypokalemia in several settings, including alcohol withdrawal, hyperthyroidism, acute myocardial infarction, and extreme head damage. Patients sometimes present with weakness of the extremities and limb girdles, with paralytic episodes that happen most incessantly between 1 and 6 a. Hypokalemia is normally profound and nearly invariably is accompanied by hypophosphatemia and hypomagnesemia. Increases in -adrenergic exercise play an important function in that high-dose propranolol (3 mg/kg) rapidly reverses the associated hypokalemia, hypophosphatemia, and paralysis. Nonrenal lack of potassium the loss of K+ in sweat is typically low besides under extremes of physical exertion. Intestinal lack of K+ because of diarrhea is a globally important cause of hypokalemia in mild of the worldwide prevalence of diarrheal disease. Renal lack of potassium Drugs can improve renal K+ excretion by a variety of different mechanisms. Diuretics are a particularly frequent trigger as a end result of associated will increase in distal tubular Na+ supply and distal tubular flow price along with secondary hyperaldosteronism. Thiazides affect plasma K+ concentration larger than that of loop diuretics regardless of their lesser natriuretic effect. Finally, a number of renal tubular toxins cause renal K+ and magnesium losing, leading to hypokalemia and hypomagnesemia; these medicine embrace aminoglycosides, amphotericin, foscarnet, cisplatin, and ifosfamide (see additionally "Magnesium Deficiency and Hypokalemia," later). In consequence, will increase in aldosterone bioactivity and/or gains in function of aldosterone-dependent signaling pathways are related to hypokalemia. Hypertension and hypokalemia as a end result of increases in circulating 11-deoxycorticosterone happen in patients with congenital adrenal hyperplasia attributable to defects in either steroid 11-hydroxylase or steroid 17-hydroxylase; poor 11-hydroxylase results in associated virilization and different signs of androgen extra, whereas decreased intercourse steroids in 17-hydroxylase deficiency result in hypogonadism. They might have an increase in urinary calcium excretion, and 20% are hypomagnesemic. Other features embody marked activation of the renin-angiotensin-aldosterone axis. Regardless of the dominant mechanism(s), hypomagnesemic sufferers are clinically refractory to K+ substitute in the absence of Mg2+ repletion. Notably, magnesium deficiency can also be a typical concomitant of hypokalemia, since many problems of the distal nephron might trigger both potassium and magnesium wasting (Chap. Bicarbonate retention and other acidbase results of hypokalemia can contribute to the technology of metabolic alkalosis. Hypokalemia additionally predisposes to acute kidney injury and may result in end-stage renal illness in sufferers with long-standing hypokalemia as a end result of eating problems and/or laxative abuse. Correction of hypokalemia is particularly essential in hypertensive patients handled with diuretics, in whom blood pressure improves with the institution of normokalemia. Diagnostic strategy the purpose for hypokalemia is often evident from historical past, bodily examination, and/or basic laboratory checks. The presence of a non-anion-gap acidosis suggests a distal, hypokalemic renal tubular acidosis or diarrhea; calculation of the urinary anion gap can help differentiate these two diagnoses. Renal K+ excretion may be assessed with a 24-h urine collection; a 24-h K+ excretion of <15 mM is indicative of an extrarenal reason for hypokalemia. The urgency of remedy depends on the severity of hypokalemia, associated clinical elements (cardiac disease, digoxin remedy, and so forth. When extreme activity of the sympathetic nervous system is believed to play a dominant position in redistributive hypokalemia, as in thyrotoxic periodic paralysis, highdose propranolol (3 mg/kg) ought to be thought of; this nonspecific -adrenergic blocker will right hypokalemia with out the chance of rebound hyperkalemia. Potassium bicarbonate or potassium citrate ought to be thought-about in patients with concomitant metabolic acidosis. Notably, hypomagnesemic patients are refractory to K+ substitute alone, so concomitant Mg2+ deficiency ought to at all times be corrected with oral or intravenous repletion. The deficit of K+ and the rate of correction should be estimated as accurately as potential; renal operate, medications, and comorbid conditions such as diabetes ought to be considered to gauge the risk of overcorrection. In the absence of abnormal K+ redistribution, the entire deficit correlates with serum K+ so that serum K+ drops by approximately zero. However, due to the issue in assessing the deficit accurately, plasma K+ focus should be monitored fastidiously during repletion. The use of intravenous administration should be limited to patients unable to make the most of the enteral route or within the setting of extreme problems (paralysis, arrhythmia, etc. Intravenous K+-Cl� ought to at all times be administered in saline solutions quite than dextrose since the dextrose-induced increase in insulin can acutely exacerbate hypokalemia. The peripheral intravenous dose is usually 20�40 mmol of K+-Cl� per liter; higher concentrations may cause localized pain from chemical phlebitis, irritation, and sclerosis. Femoral veins are preferable, since infusion by way of internal jugular or subclavian central lines can acutely increase the native concentration of K+ and affect cardiac conduction. These measures may embody minimizing the dose of non-K+-sparing diuretics, limiting Na+ consumption, and using clinically applicable combinations of nonK+-sparing and K+-sparing medications.
Order 100 mg extra super levitra visa
Management � Diagnosis the important thing diagnostic medical options of seborrheic dermatitis are pink plaques with fine greasy white scale on the scalp erectile dysfunction pump demonstration purchase extra super levitra 100 mg amex, eyebrows what if erectile dysfunction drugs don't work buy extra super levitra 100 mg on-line, nasolabial fold, and ears. Mild scalp seborrheic dermatitis can normally be controlled with over-the-counter shampoos containing zinc pyrithione (Head and Shoulders), selenium sulfide (Selsun), coal tar (Neutrogena T-Gel), salicylic acid (Neutrogena T-Sal), or ketoconazole (Nizoral A-D). Patients are typically younger adults, average age at presentation is 10 to 35 years, and females are barely extra affected (1. Several elements recommend an infectious agent based mostly on clustering of circumstances, self-limited nature, and uncommon recurrences. Herald patch with collarette scale and multiple smaller lesions with comparable morphology. Reported variants embody papular, vesicular, urticarial, purpuric, inverse pityriasis rosea, and absent or numerous herald patches. Laboratory Findings As pityriasis rosea is a medical diagnosis made by historical past and bodily examination, laboratory studies are normally unnecessary. Occasionally a viral-like constitutional prodrome or signs of an upper respiratory infection could precede the onset of cutaneous lesions. Diagnosis the necessary thing diagnostic clinical options of pityriasis rosea are an initial herald patch, an oval plaque with a collarette (scale) adopted by a symmetric, secondary eruption in a "Christmas tree" sample. The subsequent lesions are smaller (1-2 cm) pinksalmon-colored papules and plaques on the trunk and extremities. Pigmented skin alters the colour of lesions with a violet-gray shade spectrum as opposed to pink. It is extra frequent to see involvement on the top in darker pigmented people as properly. Differential Diagnosis the differential diagnosis includes different papulosquamous illnesses (Table 9-1). Other: Viral exanthems, pityriasis lichenoides chronicus, lichen planus, and erythema dyschromicans perstans. Additionally, no therapies could be recommended on the idea of evidence-based drugs. A current Cochrane evaluate showed inadequate proof for practically all interventions corresponding to emollients, topical antihistamines, steroids, light therapy, and antimicrobials. Lotions with camphor, menthol, pramoxine, or oatmeal might provide added antipruritic benefit. Use of sedating (diphenhydramine, hydroxyzine) and nonsedating (cetirizine) antihistamines can also provide relief. Medium-potency topical steroids, similar to triamcinolone or fluocinonide, might provide an additional antipruritic profit as nicely as improve the infected look of lesions. Pathophysiology Lichen planus is thought to occur because of an immune dysfunction with altered floor keratinocyte antigen presentation and subsequent cytotoxic T-cell response. The skin eruption has been associated with systemic medication and hepatitis C virus, however a definitive cause has not been recognized. Common drugs linked to lichen planus are gold, antibiotics, diuretics, and antimalarials. Clinical Presentation History Patients usually present with a complaint of itching and onset of pink bumps. The pruritus can vary from mild to severe with an occasional patient having no signs. These could also be scaly, and Indications for Consultation Severe or nonresolving case with recalcitrant pruritus. Violaceous flat-topped papules with fine white strains (Wickham striae) on flexural wrist. Management Removal of the offending agent is step one, if one is identified. Drug-induced lichen planus and hepatitis C are frequent situations that may current with a lichenoid pores and skin eruption. If corticosteroids are used for prolonged durations, care must be taken to keep away from drug-induced secondary adjustments similar to atrophy. Indications for Consultation Unusual shows or widespread distribution of a lichenoid eruption should be thought of for session. Additionally, moderate to extreme oral illness could require consultation with a specialist. The lesions are distributed symmetrically, typically on the flexor wrists, forearms, ankles, decrease again, and genitals. Scalp lesions with a scarring alopecia will be the only manifestation of the illness. This phenomenon is triggered by trauma, with resultant lichen planus observed within the area of damage. Hypertrophic lichen planus most often includes the anterior shins and the papulonodules present marked hyperkeratosis. Psoriasis remedy in tough locations: scalp, nails, and intertriginous areas. Review of remedy options for psoriasis in pregnant or lactating ladies: from the Medical Board of the National Psoriasis Foundation. Dandruff-associated Malassezia genomes reveal convergent and divergent virulence traits Laboratory Findings essentially the most useful diagnostic check is a skin biopsy. The biopsy exhibits a uniform band-like lymphocytic infiltrate at the base of the epidermis. Scabies: Presents with tiny excoriated papules and/ or vesicles in lots of the similar areas as lichen planus. Pityriasis rosea: an update with a crucial appraisal of its attainable herpes viral etiology. Effect on high quality of life in patients with pityriasis rosea: is it associated with rash severity They hardly ever trigger serious illness, however fungal infections are often recurrent or chronic in otherwise healthy people. The availability of effective over-the-counter antifungal medicines has been useful to people with actual fungal infections, but these medications are frequently used by individuals who truly produce other pores and skin ailments such as dermatitis. One of the principle diagnostic issues with fungal infections is that they carefully resemble dermatitis and different inflammatory issues. Superficial dermatophyte infections are a common reason for skin illness worldwide, particularly in tropical areas. The names of the various dermatophyte infections start with "tinea," which is a Latin term for "worm. However, the presence of toe web scale and nail plate thickening is more characteristic of a fungal infection. The other causes of nail diseases similar to psoriasis and lichen planus may seem similar to fungal infections.