Discount 1 mg detrol amex
The technique is demanding medicine abuse order detrol 1 mg fast delivery, the outcomes are variable treatment e coli buy detrol 4 mg cheap, and the anesthetic risks are larger than for the older child. This method obviates the avoidance of surgical procedure that might result from manipulation and casting. Most surgeons function on the kid between ages three and 12 months (176, 180, 213, 217). Anesthetic risks, difficulty with venous access, and the technical problem related to foot dimension are greater under age 6 months. The Cincinnati incision can be utilized for revision surgery, even crossing longitudinal scars from earlier surgical procedure. If nonetheless not aligned, the talonavicular joint capsule is released judiciously, starting medially and thoroughly progressing plantar and dorsal. Procedures that involve extra intensive capsular releases are probably to require fixation. One of the many challenges of wire fixation is the lack to precisely determine the proper alignment of the bones and joints. There is minimal ossification of the tarsal bones in infants, so the accuracy of radiographic analysis is marginal at best. Pinning in a poor alignment is perhaps as doubtless as pinning in the anatomic place. Before closure of the wound, some steps should be taken to decrease the bleeding in the foot as a result of this will cause appreciable swelling, which can necessitate splitting or removing of the cast. Approximate the subcutaneous tissues with interrupted absorbable sutures, and approximate the skin edges with a working subcuticular absorbable suture, such as 4-0 Monocryl. Apply a stable long-leg solid with the foot in the absolutely corrected position and with the knee bent 90 degrees and the thighΦoot angle set at 45 levels outward. Another long-leg cast is applied and maintained for four to 6 weeks, relying on the age of the child. After the ultimate cast is eliminated, there are alternatives for sustaining deformity correction. Another option is to use an ankleΦoot orthosis in an overcorrected place, both day and night time or at nighttime solely. In a severe clubfoot that has not responded properly to casting, it will not be potential to instantly approximate the perimeters of the Cincinnati incision with the foot in the fully corrected position without compromising the circulation of the pores and skin. It has been suggested to go away the pores and skin edges separated with the foot within the absolutely corrected position and allow for wound closure by secondary intent (220). Alternatively, the skin edges can be approximated (with or without a pin inserted across the talonavicular joint), the solid could be applied with the foot in plantar flexion, and the foot may be manipulated safely into additional dorsiflexion during a solid change beneath anesthesia 1 to 2 weeks later (175ͱ77, 219). The approach to management of a few of the postoperative deformities will now be mentioned. The incisions used for clubfoot surgery range widely and are extra quite a few than may be described here. All have been used successfully, but what is finished beneath the incision is way extra necessary to the end result than the incision itself. Turco (175) described a straight incision that ran from the bottom of the first metatarsal, underneath the medial malleolus, till it reached the Achilles tendon (A). He identified that a proximal extension of the incision along the Achilles tendon was contraindicated and that no undermining of the wound must be carried out. This transverse incision begins on the medial aspect of the foot, over the naviculocuneiform joint. From there, the incision passes posteriorly to cross simply beneath the tip of the medial malleolus. It continues across the again of the ankle a minimum of 1cm proximal to the posterior heel crease and continues laterally to move under the lateral malleolus, ending on the sinus tarsi. Although some surgeons have deserted this incision due to wound issues, many more report using it routinely without issues. Some surgeons favor to use two incisions: one posterior and one medial, with a third incision laterally over the calcaneocuboid joint, if that is necessary. The heart of the calcaneus, the front of the medial malleolus, and the bottom of the first metatarsal type a triangle. The center a part of this incision is parallel to the base of the triangle, whereas the proximal part angles towards the middle of the heel and the distal half crosses over the dorsum of the foot. The posterior incision (not shown) runs from some extent in the midline about 4 cm above the tibiotalar joint obliquely to a point midway between the Achilles tendon and the lateral malleolus. The foam head cradle utilized by anesthesiologists to assist the head serves as a superb help for the prone toddler. The foot could be raised with a folded sheet underneath it to enable higher entry to it. This is greatest accomplished by leaving the sheath attached to the subcutaneous tissue. Therefore, the incision within the pores and skin and subcutaneous tissue is carried directly down onto the tendon, passing by way of its filmy sheath. Then the tendon is exposed circumferentially by gently teasing its sheath away with a small elevator. A great amount of proximal exposure may be achieved by inserting the blade of a Senn or Langenbeck retractor proximally and pulling upward whereas "toeing in" on the retractor. With the Senn retractor elevating the skin proximally, the lateral half of the tendon is detached proximally. Sutures could be handed via the free finish of both halves to act as handles to aid with later restore. The next step is to open the deep posterior compartment, a distinct anatomic compartment that might be opened by incising it with a knife. Starting proximally, the fats beneath the Achilles tendon is sharply incised in a longitudinal straight line. As this incision is deepened, the fascial boundary of the compartment is encountered and, beneath it, extra fat in the posterior compartment. Often, after this incision is completed, the anatomic structures within the posterior compartment come instantly into view (A). In such cases the incision might come down directly over the posterior tibial nerve, as illustrated here. This structure is the primary landmark to establish within the posterior compartment and is well acknowledged as the one tendon passing behind the medial malleolus by which the muscle belly extends this low. This dissection is sustained across the medial aspect of the ankle as far as the posterior side of the medial malleolus. The dissection is facilitated by opening the sheath of the flexor hallucis longus tendon longitudinally until the sustentaculum tali is encountered. This is the purpose at which the tendon can no longer be seen and is the landmark that identifies the subtalar joint, as that joint is immediately adjacent to the sustentaculum tali.
Discount 1 mg detrol visa
One or two are passed from the cephalad to caudal path symptoms ebola 1 mg detrol otc, as in the Salter osteotomy treatment hyperthyroidism detrol 4 mg order with amex, and one other from the caudal course, close to the acetabular edge of the distal fragment, in the proximal course. She was treated for congenital dislocation of the best hip at three months of age with a closed reduction. She was handled with a triple-innominate osteotomy fastened with two 5/32-inch threaded pins. They are stronger, could be removed percutaneously with radiographic control, or may be left buried. Five years postoperatively (C), the affected person stays symptom free, with good radiographic coverage of the hip. It is among the latest of a collection of pelvic osteotomies which have been developed to enable more extensive corrections than are routinely achievable by easy innominate osteotomy in the adolescent and young adult hip. Alternatives to the Bernese (Ganz) osteotomy embody the triple-innominate osteotomy of Tonnis (422) and the spherical rotational osteotomies developed independently in Europe by Wagner (437, 438) and in Japan by Ninomiya and Tagawa (456). The greatest indication for any acetabular realigning osteotomy is a spherically congruous dysplastic hip with efficient malorientation of the acetabulum and minimal osteoarthritic changes. It could be carried out by way of a single anterior incision via an abductor sparing approach (457ʹ59). The acetabular osteotomy fragment is massive enough to have adequate vascularity to permit simultaneous arthrotomy to carry out labral debridement and other intraarticular work. The fragment can also be large sufficient to permit strong inside fixation with a quantity of screws, allowing early partial weight bearing with crutches and no exterior immobilization. Postoperatively, routine deep-venous thrombosis prophylaxis is maintained for 6 weeks in patients over 15 years of age. Postoperative ambulation is begun 48 to 72 hours after surgery, as quickly as the drains have been removed. The affected person is maintained at one-sixth physique weight bearing on the operative limb with crutches or a walker for six to 8 weeks. A recent mean 20-year follow-up has been revealed by the developer of the procedure (460). As with all acetabular procedures, solely long term follow-ups will decide if degenerative joint disease may be prevented (241). The second group among the many remedy options contains acetabuloplasties that involve incomplete cuts and hinge on totally different features of the triradiate cartilage, such because the acetabular procedures described by Pemberton (40, 344, 346, 365, 367ͳ69, 461ʹ63) and Dega (464ʹ68). These procedures can theoretically decrease the volume of the acetabulum as a result of they rely upon the triradiate cartilage because the fulcrum, although a recent paper disputes this assumption (469). First, the acetabulum was not only "shallow" but in addition going through forward and laterally. Second, in the dislocating hip, the femoral head was usually small in relation to the acetabulum, whereas within the subluxating hip the acetabulum was large relative to the femoral head. The osteotomy was designed to hinge in the acetabulum by way of the flexible triradiate cartilage. Pemberton also noticed that the path of protection obtained might be diversified, relying on the course of the osteotomy of the ilium (40). The ability to differ the course of the protection is a further advantage, especially when more lateral than anterior protection is desired. A ultimate advantage is that the bone graft is secure with out additional pins, obviating the need for subsequent pin removal. In normal youngsters, the triradiate cartilage is sufficiently mobile till 7 or 8 years of age. In children with severe cerebral palsy or myelomeningocele, in whom this is typically a useful operation, mobility in the triradiate cartilage could be present till 10 years of age or later. A mixture of the Pemberton and Salter osteotomies has additionally been described - the Pember-Sal osteotomy (470). A Pember-Sal osteotomy is used most frequently and incorrectly to describe an osteotomy that has not stayed inside the ilium but rather has broken into the sciatic notch earlier than reaching the triradiate cartilage. The patient is positioned in the same position as for open reduction of the hip joint by way of the anterior strategy, and the identical incision and method are used. Postoperatively, because of the usual young age at which this osteotomy is carried out, the patient is immobilized in a single-leg spica solid. The size of immobilization is dependent upon the opposite procedures carried out, but 6 weeks of immobilization is often sufficient to enable protected weight bearing and bodily remedy to regain movement. The patient is positioned supine on a radiolucent table with the ipsilateral leg draped free. The traditional Smith-Petersen incision, which is convex anteriorly, is extensile but usually heals with a large scar. For the more experienced surgeon, the abductor attachment to the iliac crest could additionally be left undisturbed. Only a small subgluteal window made just distal to the iliac crest is required laterally to enable the noticed cut osteotomy of the supraacetabular ilium. After the skin incision, the tensor fascia lata-sartorius interval is developed, staying lateral to protect the lateral femoral cutaneous nerve. Along the ground of this interval, the fascia over the rectus femoris is identified. Next, the exterior and inside indirect muscular tissues are reflected in a subperiosteal method off the anterior half of the iliac crest. The internal pelvis is then exposed in a subperiosteal method to the extent of the pelvic brim. The hip is then flexed and adducted, with the leg supported briefly on a towel bump under the knee and thigh. The rectus muscle and the iliocapsularis are elevated sharply collectively off the hip capsule in a medial and distal course. The psoas sheath is then opened longitudinally to permit the psoas tendon to be retracted medially, exposing the iliopectineal eminence. A spiked Hohmann retractor impacted into the superior ramus medial to the iliopectineal eminence will help in the publicity. Large Mayo scissors can be utilized to additional open the interval for the ischial reduce between the capsule and psoas on the degree of the infracotyloid groove. Confirmation with the image intensifier is helpful at this step in each the anteroposterior (A) and fake profil (B) projections (9). Once sufficient space has been created between the psoas tendon and the medial capsule, the forked tip of the Ganz chisel is placed just distal to the hip capsule but within the infracotyloid groove of the ischium. The chisel tip must remain proximal to the obturator externus tendon that lies within the groove, since the major medial femoral circumflex artery branch lies simply distal to the tendon. The blade is held perpendicular to the lengthy axis of the physique and directed in an anterior to posterior course.
Detrol 2 mg with amex
The shoulder is taken into account a ball and socket joint; nonetheless the glenoid humeral shape and measurement discrepancy described has drawn analogies to a golf ball on a tee (265) medicine lyrics buy 1 mg detrol overnight delivery. Static stabilizers include unfavorable intra-articular strain acute treatment 4 mg detrol cheap free shipping, the glenohumeral ligaments, in addition to the labrum. The superior, center, and inferior glenohumeral ligaments provide anterior stability. The superior glenohumeral ligament plays a role in providing inferior stability and the anterior band of the inferior glenohumeral ligament is a significant stabilizer with the shoulder in an kidnapped and externally rotated place. Dynamic stabilizers embrace the rotator cuff and the lengthy head of the biceps tendon which contribute to joint compression. In addition to the rotator cuff and biceps, the deltoid and scapulothoracic muscle tissue position the scapula to present maximum stability on the glenohumeral joint. Traumatic dislocations in youngsters happen with the same mechanism as those seen in adults, together with forced abduction and external rotation accidents throughout contact sports activities in addition to vital falls onto an outstretched hand. However, if the affected person is seen a quantity of weeks after the inciting occasion, the radiographs may be misinterpreted as displaying a neoplasm or an infection. The beneficial remedy of sufferers with pelvic avulsion fractures has generally been rest, adopted by a particular rehabilitation program. Metzmaker and Pappas (256) outlined a five-stage rehabilitation program that consists of rest to loosen up the concerned muscle groups as well as ice wrap and analgesics, initiation of mild active and passive movement, resistance workouts after 75% of movement is regained, stretching and strengthening workouts with an emphasis on sports-specific workout routines, and at last return to competitive sports. Surgical intervention with makes an attempt at open reduction and internal fixation has been recommended for isolated incidents, however there seems to be no superiority of operative intervention over conservative management (256). Patients should be advised that the anticipate return to competitive athletics could also be prolonged. There are two broad classes of dislocation which embody traumatic or atraumatic. This widely used classification system is that of Rockwood (266) who famous that of forty four circumstances of dislocation, 8 have been traumatic and 36 have been atraumatic (Table 31-3). Anteroposterior radiograph of right hip demonstrating how avulsion fracture of ischium may be mistaken for neoplasm or an infection. A child with an acute traumatic anterior shoulder dislocation could present with the arm held in slight abduction and exterior rotation. With traumatic posterior dislocation, the arm is held adducted and in marked inside rotation and the humeral head could also be palpated posteriorly. With either dislocation, the traditional rounded contour of the shoulder is lost, and any try to move the shoulder either actively or passively is often very painful. A cautious history and bodily exam are vital to the prognosis in the analysis of isolated and recurrent episodes, particularly in the young athlete. Patients incessantly recall a selected traumatic event in addition to a reduction maneuver occurring spontaneously or with assistance. The clinician ought to report whether or not the shoulder grew to become relocated on the scene of the harm or within the emergency room. These sufferers may also describe multiple instructions of translation with anterior and posterior subluxation or dislocation being extra frequent than inferior. The bodily examination consists of an evaluation of active and passive vary of motion, in addition to shoulder and upper arm energy. Most essential for the assessment of instability are the analysis of translation of the humeral head on the glenoid and apprehension and relocation testing. The stability examination ought to include an evaluation of each shoulders to find a way to distinguish pathologic laxity from physiologic laxity. The shoulder examination should also embody a whole examination of the cervical backbone. Glenohumeral stability may be assessed with the affected person within the sitting or supine place. The sitting position requires a relaxed cooperative affected person, however the supine place is often preferred, especially with provocative tests for dislocation. Translation of the humeral head is first evaluated with the shoulder in the neutral place, in exterior rotation for anterior inferior testing, and in flexion and internal rotation for posterior inferior translation. The quantity of translation in every path is quantified and in comparison with the healthy shoulder. These are sometimes referred to as apprehension exams and reproduce the mechanism of instability (dislocation) that the patient acknowledges. The anterior apprehension test is performed by abducting and externally rotating the shoulder ninety levels in each direction. As extra pressure is gently utilized, the athlete will turn into apprehensive of an impending dislocation and both adduct and internally rotate the shoulder or show their concern by altering facial expression or by making a sound. For the posterior apprehension check, the shoulder is flexed to ninety degrees and internally rotated with a posterior pressure applied to the shoulder joint by way of the upper extremity. After the anterior apprehension check has been performed, a hand is positioned anteriorly over the upper humerus and a posteriorly directed drive is utilized while once more performing the apprehension take a look at. The posterior relocation check is completed within the opposite method, with a handheld over the posterior side of the upper humerus (applying an anteriorly directed force) whereas the posterior apprehension take a look at is performed. With the affected person sitting, the humerus is grasped distally just above the elbow, and an inferiorly directed force is applied while stabilizing the scapula. A dimple or hole will seem over the lateral shoulder because the humeral head is translated inferiorly. If the athlete has two or more of these signs, the diagnoses and implications of generalized ligamentous laxity should be thought-about. Prereduction films must be taken in most sufferers to affirm the direction of the dislocation and to rule out fracture. However, the prognosis of anterior dislocation is quickly apparent with the hurt held in slight abduction and exterior rotation with the humeral head palpable anteriorly. If the treating doctor is skilled in diagnosis and administration, discount of the dislocation with out prior x-rays is permitted. On the playing field, that is completed by light traction on the arm in slight abduction, ahead flexion, and internal rotation previous to the onset of muscle spasm. In the emergency room, discount is best accomplished by acceptable sedation and placing the affected person prone, with the arm hanging free and 5 to 10 lb (2 to 5 kg) of weight hooked up to the higher extremity. Therapy must be aimed at restoration of motion and then a selected strengthening program. The athlete ought to work vigorously on the anterior rotator cuff (supraspinatus and subscapularis) in addition to on the periscapular muscular tissues following an anterior dislocation. In the rare case of a posterior dislocation, the posterior rotator cuff muscles or exterior rotators (infraspinatus and teres minor) ought to be isolated and strengthened. In seated position, the affected person lifts his or her boy from a chair by putting the palms on the chair and lengthening the higher extremities. Elevation of the arm within the scapular plan with the arm internally rotated and thumbs pointed down. In addition to restorative motion and strengthening workouts, nonoperative treatment for first-time dislocators has classically been preceded by several weeks of immobilization in internal rotation. It has been famous by some that when the arm is immobilized in exterior rotation, the Bankart lesion is more accurately positioned along the glenoid rim to guarantee proper anatomic healing, thereby reducing the probability of redislocation (270Ͳ72). Patient immobilized in exterior rotation brace after acute anterior glenohumeral dislocation (A).
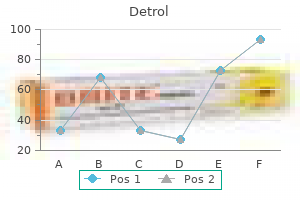
| Comparative prices of Detrol |
| # | Retailer | Average price |
| 1 | Safeway | 396 |
| 2 | BJ'S Wholesale Club | 798 |
| 3 | Subway | 198 |
| 4 | DineEquity | 517 |
| 5 | GameStop | 554 |
| 6 | Tractor Supply Co. | 214 |
Detrol 1 mg discount on line
These osteotomies may be difficult in these very large treatment bladder infection detrol 2 mg buy online, heavy sufferers with important deformity useless id symptoms cheap detrol 4 mg without a prescription. Intertrochanteric osteotomies are also somewhat limited in their capacity to right the deformity due to their appreciable distance from the location of deformity. In asymptomatic patients with severely affected slips, the role of osteotomy is unclear. A 13-year-old woman presented with pain on sitting and issue riding a bike because of exterior rotation of the left hip sixteen months following in situ fixation. Anteroposterior pelvis (A) and lateral (B) radiographs of the left hip show the residual deformity 16 months following pinning. Lateral x-ray film exhibits the proximal femoral metaphysis articulating with the acetabulum preoperatively. Sugioka famous postoperative valgus in three hips that had marked deformity preoperatively. Another sequence of five hips has been described, with problems in two patients (40%) (330). Although the outcomes with this method appear promising, the method is demanding, complications are frequent, and its use has been reported in only some centers. Most commonly, these embrace hip and/or groin pain with extended sitting (owing to femoral neck impingement on the acetabulum) and practical limitations as a result of lack of the hip vary of movement. Although such indicators and symptoms are widespread in the first few months following in situ fixation, they usually enhance inside 1 yr of pinning. This is usually a Southwick osteotomy, with valgus, flexion, and inner rotation. He thinks that the risks of such osteotomies in asymptomatic sufferers are too great relative to the uncertain potential for long-term gains, particularly given the anticipated ongoing advances within the fields of orthopaedics and basic science in the course of the lifetime of these kids. In addition, asymptomatic patients who bear proximal femoral osteotomy are generally made clinically worse for a minimal of the first 6 months following a proximal femoral osteotomy. The proximal femoral osteoplasty will decrease the need for an intertrochanteric correction and hence will decrease the shortening effect on the limb. Performing an Intertrochanteric Osteotomy Through a Surgical Dislocation Approach permits the ability to examine the joint and carry out a proximal femoral osteoplasty (A). The trochanter osteotomy and the femoral osteotomy are mounted simultaneously with a blade plate. Panels (F) and (G) are the postoperative radiographs after a flexion intertrochanteric osteotomy carried out via a surgical dislocation approach. Recent authors have attempted to weigh the risks and benefits and their recommendations are conflicting. Opponents of prophylactic pinning cite the issues of prophylactic therapy, noting the potential dangers of pinning quite a few hips that will by no means slip, and likewise pointing out that with applicable affected person counseling and shut follow-up most subsequent slips will be detected while still delicate. In one research of ninety four hips handled with prophylactic pinning, there have been no complications (9). It can be inferred from these information that the probability of a contralateral slip first being recognized after adolescence is 25% to 30%. For a given diploma of misdirection, the biomechanical alignment and eccentricity in the femoral head will be worse for a light slip (A) than will in all probability be for a extra severe slip (B) because of the longer distance the screw must traverse in a light slip. Further, Hagglund famous that no hip with a light or moderate slip handled with in situ pinning developed arthritis before the age of 50 years. Prophylactic pinning ought to be carried out for children with underlying endocrine illness due to their excessive rate of contralateral slip. Previous pelvic radiation, which included the contralateral hip within the field, is another indication for prophylactic pinning. In kids with renal disease, medical management somewhat than prophylactic pinning is beneficial. At the time of re-presentation, anteroposterior (C) and frog lateral (D) radiographs show marked slip of the beforehand regular right hip. Femoral neck osteoplasty entails removal of the distinguished anterosuperior femoral neck and could additionally be performed alone or together with different procedures, similar to proximal femoral osteotomies (124, 342, 343). Symptoms that may suggest the potential good factor about osteoplasty include pain on sitting caused by the impingement with hip flexion. If carried out in isolation, osteoplasty leaves unchanged the irregular relation between the femoral head, neck, and shaft, with relative retroversion, extension, and varus. Previous authors have famous that osteoplasty might additional improve hip vary of motion following intertrochanteric osteotomies (124, 342, 343). Hall (275) noted that complications had been the one issue that seemed to result in an early poor end result. At a imply follow-up of forty one years, Carney and Weinstein (167) reported Iowa hip scores of no less than eighty in 26 of 31 hips (84%). Hagglund (269) noted that no hip with a gentle or average slip handled with in situ pinning developed arthritis before 50 years of age. Recent authors have sought to prevent late arthritis by restoring more normal proximal femoral anatomy by performing proximal femoral redirectional osteotomies (89, 292). In these two series, the overall breakdown of slips was 76% chronic, 21% acute-on-chronic, and 3% acute. The combination of anti-inflammatory drugs, bodily remedy, and protected weight bearing may be useful in maintaining the vary of movement and preventing progressive femoral head collapse. When femoral head collapse occurs within the space of beforehand positioned screws, the screws should usually be backed out or removed to be able to stop joint penetration and chondrolysis. With progressive collapse and joint degeneration, salvage procedures are often essential. Impact actions similar to running, leaping, and ball sports should be averted, whereas swimming and bicycling may be undertaken to keep cardiovascular health, energy, and vary of movement. Anti-inflammatory drugs and ambulatory aids could also be beneficial as properly, though these are often rejected by in any other case healthy adolescents and younger adults. Normal cartilage thickness of the pediatric hip has been reported to decrease from a imply of 6 mm in children aged 1 to 7 years, to 5 mm in these aged eight to 12 years, and to four mm in those aged 13 to 17 years (355). Unlike many different hip maladies, chondrolysis causes the hip to be held in abduction and ultimately ends in a onerous and fast abduction contracture. Chondrolysis is extra widespread within the feminine population than in the male population (243, 245, 359). Previously, chondrolysis was believed to be more widespread in black children (76, 180, 212, 243, 356, 360), although more recent studies have refuted this assertion (202, 216, 243, 360, 361). One series reported a better incidence of chondrolysis in those of Hawaiian descent (357). Ten months later, the affected person offered to the office with a 1-month historical past of left hip ache. However, 2 months postoperatively the patient began to have elevated hip ache, issue walking, and decreased hip vary of movement. Chondrolysis is seen following all types of remedy and has also been reported to be present at the time of preliminary presentation in some patients (243, 245). Maurer and Larsen (357) instructed that chondrolysis was extra widespread with severe slips and with spica casting, open reduction, or extended casting.
Order detrol 2 mg line
Older children need to medicine pill identification generic detrol 1 mg with visa be taught methods to become impartial in donning and doffing the prosthesis treatment diabetes 4 mg detrol trusted, toileting, and other activities with the prosthesis. Fitting of a new prosthetic part, for example, a hydraulic knee joint, will usually require particular training to maximize the benefits of the model new elements. Adaptations for sports activities, for instance, special terminal devices, if desired, or a swimming leg, are necessary, as is the advocacy role to allow the youngsters to take part in all possible actions. In adolescence, the necessity for specific therapeutic interventions is usually minimal. The youngster has now turn out to be totally aware of his or her differences and their significance. Appearance being important, extra cosmetic prostheses and improved gait turn out to be important points. The therapist can play a crucial function in directing the child and oldsters to the suitable company for the foundations of the state, and to a supply for analysis and modifications to the automobile. As with any adolescent, the amputee ought to attend driver training training, using modifications if needed. Switching the brake and gasoline pedals to accommodate unilateral decrease limb loss is doubtless considered one of the most typical examples. Many amputees, even with bilateral decrease extremity loss, drive with out adaptations. A ring adaptation can be utilized to modify the steering wheel for upper extremity amputees. The larger level amputee, and those with multilevel limb loss, may profit from a handicap parking license. The therapist may be of nice worth in assessing the scenario, counseling the affected person, and serving to with the transition. The Internet can prove to be a fantastic resource in assisting college-bound students and their households. Learning to toss a ball, jump, run, hop, and experience a bicycle are actions included on standardized developmental screenings and checks. Recreational and sports-related terminal devices can be found for the upper extremity amputee (232, 233). Adaptations may be as simple as elevating the handlebars on a bicycle and adding a toe strap to highly subtle prosthetic parts specific to each sport (234). Information and resources for sports activities and adaptive recreation for the amputee could be obtained via the Amputee Coalition of America. Improving self-esteem and confidence, gaining independence, learning to win and lose, growing decision-making and problem-solving skills, and cooperating as a group member are a number of of the advantages that a child carries throughout his or her life. Improving physical health, developing steadiness, power, coordination and motor expertise, rising endurance, and weight management are advantages of bodily activity. Over the years, there was an elevated consciousness of adapted sports and recreation for people with bodily and psychological impairments. The Paralympic and Special Olympics initiatives have been the most obvious and have sparked a rise in availability of applications for special-needs kids. Laws also have been handed for children to receive schooling in the least restrictive environments. Physical therapy and recreation are related providers included on this legislation. As seen on this photograph, participation in highlevel sports is possible for kids and adolescents with limb deficiency. Advances in prosthetic modifications design and national organizations that promote athletics give patients the freedom to pursue a broad selection of winter and summer sports activities. International forum: International Standards Organisation terminology: software to prosthetics and orthotics. Congenital abnormalities associated with limb deficiency defects: a population study based mostly on instances from the Hungarian Congenital Malformation Registry (1975ͱ984). Subclavian artery provide disruption sequence: speculation of a vascular etiology for Poland, Klippel-Feil, and Mobius anomalies. A population-based research of survival and childbearing amongst female subjects with birth defects and the chance of recurrence of their children. Vascular etiology of limb defects: the subclavian artery provide disruption sequence. Coping when a baby has a disability: exploring the impact of parent-to father or mother support. Physical attractiveness as a correlate of peer standing and social competence in preschool youngsters. Effects of stress, social support, and vanity on melancholy in youngsters with limb deficiencies. Correlates of perceived physical look in youngsters with congenital/acquired limb deficiencies. The morphology, natural history, and treatment of proximal femoral focal deficiency. Congenital short femur: clinical, genetic and epidemiological comparison of the naturally occurring situation with that caused by thalidomide. Congenital longitudinal deficiency of the fibula: follow-up of therapy by Syme amputation. Amputation in children: a follow-up of seventy four kids whose decrease extremities were amputated. The autologous stump plasty: treatment for bony overgrowth within the juvenile amputees. Tumors of the top of the fibula: good operate after resection without ligament reconstruction in 6 patients. Outcomes of lengthening short lower-extremity amputation stumps with planar fixators. A randomised double blind trial of the effect of pre-emptive epidural ketamine on persistent ache after lower limb amputation. The impact of intra-neural native anaesthetic infusion on pain following major lower limb amputation. Gabapentin in phantom limb pain management in children and young adults: report of seven circumstances. Congenital abnormalities of the femur and related decrease extremity malformations: classification and treatment. Congenital ball-and-socket ankle joints and associated lower-extremity malformations. Syme amputation; an analysis of the physical and psychological operate in young patients. Amputation and prosthesis as definitive remedy in congenital absence of the fibular. Congenital absence of the fibula: treatment by Syme amputation - indications and approach.
Generic detrol 1 mg free shipping
Associated components which will contribute to this condition embrace a broad pelvis symptoms of kidney stones generic detrol 2 mg mastercard, leg-length discrepancy treatment dvt buy discount detrol 1 mg online, and excessive pronation of the foot (362). Military recruits have offered a wealth of data relating to a cohort of comparatively younger healthy energetic participants. A potential research was carried out on Israeli male recruits aged 17 to 26, and of these 783 recruits, the risk for stress fractures was inversely proportional to age. Each 12 months, above the age of 17, the danger for stress fractures was noted to have been lowered by 28% (367). A retrospective evaluation was carried out on 154 navy patients aged 17 to 29, and of the 143 stress fractures identified 99% had been situated at the tibia (368). Many elements have been correlated with stress injuries in pediatric athletes including an excessive fee of exercise progression, anatomic malalignment, a historical past of stress accidents, changes in strength and adaptability related to development, and elevated physique mass index (366). A wellunderstood danger for stress fractures is a fast increase in training depth which may be commonly found in young athletes implementing new training protocols or beginning staff preseason training regimens. The female athlete triad of menstrual irregularity, osteopenia, and disordered consuming ought to alert the treating physician to the potential for an elevated risk for stress injuries. A distinction was famous in cumulative stress fractures with an incidence of 4% in women with a regular menstrual historical past versus 15% in ladies with irregular or absent menses (369). A potential, multicenter cohort research was carried out to examine risk components, and among 146 collegiate athletes these extra more likely to develop medial tibial stress Stress Fractures. Stress fractures are becoming more common in kids due to an increased degree of participation in organized athletics, earlier sports activities specialization, yearround sports, and participation in a quantity of groups throughout the identical season. Stress fractures come up from repeated submaximal stresses applied to regular bone or regular stresses applied to abnormal bone and can present as a spectrum spanning from a light microfracture to a whole fracture. In a research of adolescent athletes with open physes, sufferers have been primarily handled with reduction in weight bearing; nevertheless, 7 of 21 sufferers reported unsatisfactory outcomes and four patients with tibial stress fractures had persistent symptoms and had been changed from reduced weight bearing to plaster cast immobilization. Risk elements for tibial stress fractures include hip exterior rotation, knee malalignment, smaller tibial width, a poor degree of conditioning, hard terrain, as well as nutritional components. The main concern in analysis is differentiating a stress fracture from a malignant bone tumor, especially with some periosteal new bone formation. The physician must additionally rule out different conditions corresponding to benign tumors including osteoid osteoma, an infection, inflammatory arthritis, or soft-tissue harm. Shin splints are discomfort in the leg from musculotendinous inflammation on account of repetitive impression workout routines or the use of foot flexors in sports activities such as working. In patients with proximal discomfort, the examiner should verify for referred ache from the patellofemoral area as patients with the terrible triad of femoral anteversion, genu valgum, and pes planus. This terrible triad of malalignment issues is a predisposing factor in the improvement of overuse injuries of the patellofemoral region and the lower legs. When assessing a young athlete in whom an overuse harm is suspected a cautious and detailed historical past is essential in differentiating stress fractures from different situations. Night pain is uncommon in stress fractures but is frequent is osteoid osteoma or malignant bone tumors such as osteogenic and Ewing sarcoma. The bodily examination should embrace an evaluation of the complete kinetic chain together with alignment, gait, limb size, muscle strength, and flexibility which can reveal tightness, appropriate flexibility, or pathologic laxity. Stress fractures are famous to occur more generally in athletes with foot abnormalities corresponding to pes cavus and pes planus (366, 371ͳ73). Technetium scans are helpful to verify the analysis of a stress fracture, and adjustments may be famous utilizing this system as early as 12 to 15 days following the onset of harm and signs. It can at occasions be challenging using bone scintigraphy to distinguish the difference between a stress fracture of the bone and shin splints from musculotendinous inflammation. The activity modification includes education and instruction for the younger athlete to partake in train that does impart forces on the injured area. This at instances consists of eliminating the sport that the athlete participates in altogether. Bracing for lower extremity stress fractures could include boot or forged immobilization or off-the-counter orthotics for 4 to 6 weeks to enable adequate bone deposition to happen. Continued rehabilitation and prevention consists of development to strengthening, flexibility workouts and coaching, in addition to instruction concerning already addressed elements in the workup together with dietary influences, graduated coaching regimen increases, and an awareness of coaching surfaces. There are some anatomical areas which may be susceptible to prolonged signs or in some cases nonunion including the femoral neck, tibial diaphysis, medial malleolus, and tarsal navicular (366). Femoral shaft stress fractures are at low risk of nonunion or displacement and may be managed with activity modification. Surgical remedy is therefore recommended and is mostly performed with cannulated compression screws. For tibial stress fractures, the posterior medial compression facet stress fracture is the most typical. This is a low-risk stress fracture and most heal with four to 6 weeks of pneumatic boot immobilization. The tibial anterior rigidity aspect fracture is less widespread; nonetheless in this hypovascular region, callus is usually not shaped and sufferers are in danger for delayed union or nonunion (378). In the case of delayed union, a patellar tendon-bearing forged or business orthosis must be employed for four to 6 months before surgery is taken into account. If nonunion exists in the skeletally mature adolescent, choices to deal with the nonunion embody the utilization of an intramedullary nail with or with out bone grafting and fibular osteotomy (379). In the skeletally immature particular person with a diaphyseal tibial stress fracture that fails to heal after 6 months of nonoperative remedy, operative remedy is indicated. Excision of the fibrous nonunion and autogenous bone grafting from the iliac crest with attainable fibular osteotomy has been employed successfully on this uncommon situation (379). For medial malleolus stress fractures, the fracture line tends to traverse in an oblique method from the intersection of the medial malleolus and the tibial plafond. Nonoperative administration including restricted weight bearing as properly as casting or bracing has a better failure fee than different low-risk fractures. Operative intervention subsequently can be performed to facilitate early therapeutic and restoration. In the case of nonunion of tarsal navicular stress fractures, really helpful remedy consists of excision of the nonunion web site and autogenous bone grafting. In the case of 5th metatarsal fracture nonunion, really helpful remedy includes intramedullary screw fixation with or with out bone grafting. While the best concern for a young athlete is the timeliness of return to sports activities, the treating doctor should assess multiple variables. Return to play ought to be guided by components indicative of healing and injury prevention together with the cessation of ache, radiographic proof of a healed fracture, elimination of inciting causes and instruction relating to training methods, and a graduated exercise program. Sever calcaneal apophysitis is a self-limited inflammatory situation of the os calcis in rising youngsters. The typical child with Sever disease is from 9 to 14 years of age and involved in working sports activities (380). The condition is bilateral typically and presents as diffuse pain and tenderness over the prominence of the heel somewhat than exclusively on the plantar aspect as is seen in plantar fasciitis (381). With rest, activity modification, and passage of time, the condition always resolves (380, 382, 383). Cast immobilization may hardly ever be necessary for the affected person with extreme, incapacitating signs (383). Repetitive stress within the upper extremity could lead to a particular stress response in the physis.
Detrol 4 mg purchase amex
This joint is found by directing the scissors distally towards the first metatarsal between the neck of the talus and the navicular (A) medicine 54 357 cheap detrol 2 mg amex. The error is to minimize transversely across the foot as if the anatomic relationship between the navicular and the talus had been normal medications without doctors prescription order detrol 1 mg fast delivery. At the identical time, the surgeon must be careful to avoid opening the naviculocuneiform joint. This will additional devascularize the navicular and tend to destabilize it permitting it to rotate out of position. The talonavicular joint capsule must be released primarily on the medial and plantar features, as those are probably the most contracted portions. The dorsomedial capsule must be released only to the extent that it limits eversion of the subtalar joint. Excessive release of the talonavicular joint capsule would possibly lead to hypermobility and dorsal subluxation of the navicular, a tough state of affairs from which to get well. To free it, the plantar calcaneonavicular (spring) ligament and the anterior portion of the deltoid ligament inserting into the navicular (tibionavicular ligament) have to be divided. Because these ligaments are condensations of the capsules, they will be divided when the capsules between the talus and the navicular dorsomedially and the calcaneus and the cuboid on the plantar facet are opened. This could be done with a scissors or a knife when the surgeon is for certain that he or she has recognized the joint. Plantar and lateral to the talonavicular joint, and virtually according to it, is the medial aspect of the calcaneocuboid joint (B). Because the peroneus longus tendon crosses probably the most plantar and lateral side of this joint, it should be retracted. The medial capsule of the calcaneocuboid joint, like all the other capsules, could be opened safely with a scissors, although some skilled surgeons choose to use a knife. This must be carried out after the completion of the whole release and after the foot is lowered. The tendon may be repaired finish to finish with a Kessler type of sew or aspect to side. The restore should be underneath modest rigidity to avoid unnecessary weakening of the gastrocnemius muscle. In the older baby, one or more osteotomies could additionally be necessary to correct residual deformities which would possibly be recognized after the joints are aligned by soft-tissue releases. Residual midfoot adduction and supination are often a problem after clubfoot correction. In the past, painful midfoot adduction was usually handled by metatarsal osteotomies (459, 460) or tarsometatarsal capsulotomies (Hyman-Herndon procedure) (456). More recently, however, these operations have been used much less regularly because they both fail to present the desired correction or they lead to painful stiff joints (457, 458, 461, 462). The alternative is dependent upon the radiographically decided site(s) of deformity and the age of the child. In residual adductus deformities of the forefoot, the medial cuneiform is usually trapezoid shaped with medial deviation of the primary metatarsalΣuneiform joint. A bolster is placed beneath the buttocks, turning the leg internally to facilitate the approach to the cuboid. The incision may be both oblique, following the skin lines directly over the cuboid, or curvilinear over the bone. After opening the pores and skin, the peroneus brevis is recognized, free of its sheath, and retracted plantarward. The gentle tissues are freed dorsally and plantarward to expose the cuboid bone extraperiosteally, preserving the joint capsules intact. Using a microsagittal saw, a laterally primarily based wedge of bone of the specified measurement is eliminated. It is necessary to go through the medial cortex of the bone in order that the osteotomy is mobile and straightforward to shut. The wound is left open, and the bolster is eliminated to present better access to the cuneiform bone on the medial side of the foot. As the dissection is deepened, the anterior tibial tendon might be identified coursing over the primary cuneiform bone. This tendon could be dissected free with out disturbing any of its essential attachments. The dissection is started on the inferior side of the tendon, and the tendon is mirrored dorsally. In the idiopathic kind of forefoot adduction, this tendon will appear to have minimize a groove of variable depth into the bone (B). Dissection of the cuneiform bone is continued extraperiosteally until both the anterior and posterior joints are recognized positively, whereas trying to protect intact the joint capsules and while the plantar and dorsal elements are exposed. Because of the peculiar form of the first cuneiform bone in this condition, it might be sensible to examine the trail of the proposed osteotomy with the picture intensifier. Using the microsagittal saw, a single osteotomy minimize is made in the first cuneiform bone. Start half way between the anterior and posterior ends of the bone on the medial facet and, while chopping laterally, angle slightly distally. After finishing the osteotomy, an osteotome is inserted to spread apart the fragments and ensure their mobility. The graft that was taken from the cuboid is now inserted into the osteotomy of the primary cuneiform. Kirschner wires are placed into the fragments and used as pleasure sticks to open the osteotomy. It may be necessary to release the abductor hallucis tendon if it is tight or produces adduction of the great toe after the graft is inserted. The cuboid osteotomy can be manipulated, closed, and held with one or two small staples or a Kirschner wire. After the injuries are closed and dressed, the affected person is positioned in a nonηeight-bearing cast. In older children, a short-leg weightbearing cast is utilized and used for a further 2 weeks. Although quite a few methods have been described to shorten the lateral column of the foot, four receive the widest use. The first three (A-C) can be used to align an adducted navicular on the top of the talus when the subtalar joint is rigidly inverted. He beneficial shortening the lateral column of the foot by excising a portion from all sides of the calcaneocuboid joint. The defect created by the wedge is held closed by staples and is intended to end in fusion (A). There can be a risk that the foot might develop into abduction and eversion if the operation is carried out beneath age 8 years. The Lichtblau process relies on the belief that adaptive changes in the calcaneocuboid joint are what forestall sufficient discount (226). The operation, which is beneficial for children over 2 years of age, excises a laterally based mostly wedge from the anterior end of the calcaneus. A less commonly used approach for shortening the lateral column of the foot and thereby aligning the talonavicular joint is a closing wedge osteotomy of the anterior calcaneus (C).
Detrol 2 mg discount
Fluoroscopic help is utilized to confirm anatomic discount medicine names quality 2 mg detrol, information appropriate wire orientation symptoms 9 days past iui cheap detrol 4 mg visa, and keep away from the proximal tibial physis. Postoperatively, patients are placed in a postoperative hinged knee brace and maintained touchdown weight bearing for six weeks postoperatively. Motion is restricted to zero to 30 levels for the primary 2 weeks, zero to 90 degrees for the next 2 weeks, and then full range of movement. Cast immobilization in 20 to 30 levels of flexion for 4 weeks postoperatively could additionally be essential in youthful kids unable to comply with protected weight-bearing and brace immobilization. Physical remedy is utilized to obtain movement, energy, and sport-specific coaching. Patients are typically allowed to return to sports at 12 to sixteen weeks postoperatively relying on knee operate and strength. Arthroscopic setup and examination is just like the method described for epiphyseal screw fixation. Arthroscopic discount and insertion of cannulated screw inside fixation for a displaced tibial spine fracture. Type three tibial spine fracture handled with arthroscopic reduction and screw fixation. Treatment of a type 2 tibial spine fracture with arthroscopic discount and suture fixation. The information wires will traverse the tibial physis, however no circumstances of development arrest after suture fixation have been reported. The sutures are retrieved through the tibial tubercle incision, and the sutures are tied down onto the tibia. When managing tibial eminence fractures with closed discount, follow-up radiographs should be obtained at 1 and a pair of weeks postinjury to verify upkeep of discount. Type 2 tibial spine fracture handled with arthroscopic reduction and suture fixation. The injection of local anesthetic beneath sterile situations may be useful to minimize ache and allow for full knee extension in makes an attempt at closed discount. During arthroscopic reduction and fixation of tibial spine fractures, visualization may be troublesome until the massive hematoma is evacuated prior to the introduction of the arthroscope and bleeding from the fracture is managed. Adequate influx and outflow is crucial for proper visualization, and we routinely use an arthroscopic pump and a tourniquet to achieve this. Careful consideration should be paid to put together the fracture bed to present optimal conditions for bony healing. Epiphyseal cannulated screw fixation of small or comminuted tibial eminence fragments can fail as a outcome of inadequate bony purchase or additional comminution; in these circumstances, suture fixation is most well-liked. Early mobilization is helpful to avoid arthrofibrosis which might occur with immobilization. However, in younger children, compliance with protected weight bearing and brace use can be problematic, and so they have to be casted. The total prognosis of tibial eminence fractures is nice to excellent if satisfactory reduction is achieved as proven in most research. However, some studies have found no distinction within the consequence of displaced tibial backbone fractures handled closed versus open or arthroscopic (112, 114, 117, 119, a hundred and twenty, 154). A majority of research have found residual laxity of the knee after open or closed remedy for all tibial eminence fracture varieties as much as 6 mm compared to the contralateral facet (104, a hundred and five, a hundred and ten, 114, one hundred fifteen, one hundred twenty, 124ͱ26, 154). Baxter and Wiley (114, 119) discovered wonderful practical outcomes without symptomatic instability in 17 pediatric knees with displaced tibial spine fractures, despite a constructive Lachman examination in 51% of patients and elevated measured imply knee laxity as a lot as 3. In a research of 12 pediatric knees present process open reduction and inside fixation, Smith discovered subluxation signs in two sufferers despite optimistic Lachman examinations in 87% of patients (131). This laxity is worse with sort three accidents, pedestrian motorized vehicle trauma, or with different associated ligament tears (104, one hundred and five, a hundred and ten, 114, a hundred and fifteen, one hundred twenty, 124ͱ26, 154). Poor outcomes might occur after eminence fractures related to unrecognized injuries to the collateral ligaments or physeal fracture (131, one hundred fifty five, 156). In addition, hardware across the proximal tibial physis may result in a development disturbance with a recurvatum deformity (129). Malunion of type 2 and three fractures may cause bony impingement of the knee throughout full extension (126, 157). Nonunion of type 2 and 3 tibial spine fractures handled closed can usually be managed by arthroscopic or open reduction with inner fixation with or without bone graft (133, 158, 159). Debridement of the fracture mattress and the fracture fragment to bleeding bone is essential to optimize bony healing, and bone graft could additionally be required in some instances. Arthrofibrosis, notably, loss of extension, can happen after tibial backbone fracture, even after anatomic discount (132). This is assumed to be as a outcome of the local increase in blood supply during healing, which results in spine enlargement or arthrofibrosis which may trigger a mechanical block to extension. Early range of motion and mobilization is important to attempt to forestall lack of movement. Dynamic splinting and aggressive physical therapy can be employed during the first 3 months from fracture if stiffness is current. If stiffness persists after 3 months, a manipulation underneath anesthesia and a lysis of adhesions could be carried out. Overly vigorous manipulation ought to be prevented to have the ability to avert injury to the proximal tibial or distal femoral physis. The knee is the most common site of injury in the skeletally immature athlete (160). Nonoperative administration can lead to useful instability and problem with chopping and pivoting sports. Additionally, the pathologic shear forces are related to meniscal and chondral injury over time. Prior to the 1980s, these injuries had been thought to be uncommon within the pediatric athlete. The outcomes of nonoperative management in youngsters are persistently related to poor outcomes (162, 163). At ultimate follow-up, meniscal tears were current in 15 knees, three osteochondral fractures occurred, and osteoarthritic changes developed in 10 knees. Only seven patients returned to sports, all experiencing recurrent episodes of giving means, effusions, and pain. Attempts at primary repair of the ligament in youngsters have resulted in poor outcomes (164). Failure of main repair has led to the development of quite so much of procedures to stabilize the knee. Surgical choices embrace transphyseal, partial transphyseal, and physeal-sparing reconstructions. It is essential to perceive the different sorts of injuries that can occur within the skeletally immature patient. The findings on bodily exam are depending on the timing in relation to the damage.