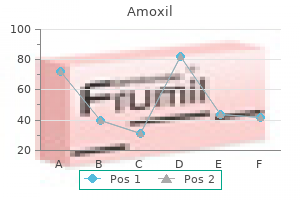
Amoxil 250 mg on-line
A scleral depressor is pressed against the lateral side of the attention in order that the attention is compressed in opposition to the medial orbital wall antibiotic starts with c buy discount amoxil 250 mg on-line. This raises the intraocular pressure antibiotics natural 500 mg amoxil purchase mastercard, augmenting fluid egress and stretching the scleral wall. In addition to making certain patency of the central retinal artery, the ophthalmoscope is used to rule out the attainable problems of anterior fuel entrapment or fish egg bubbles. Once patency of the central retinal artery has been reestablished, the outflow of aqueous is more than sufficient to compensate for the growth of the gas bubble in nonglaucomatous eyes. Accordingly, we no longer verify postoperative pressures except extreme glaucoma is present. By persevering with to press on the eye and very progressively withdrawing the needle over a quantity of minutes, one can normally remove one other zero. Highly myopic eyes are likely to have extra ample anterior chambers, however in addition they name for a larger intraocular gasoline bubble. When performing paracentesis by way of the pars plana in a pseudophakic eye, the plunger is left in the syringe to prevent occlusion of the needle with vitreous. Instructing the Patient the eye is irrigated to rinse out the povidone-iodine, an antibiotic-steroid ointment is instilled, and the attention is patched. The axis of the retinal break is marked with an arrow on the bandage, and the head is tilted so that the arrow factors toward the ceiling. Alternatively, a commercially produced "pneumo-level" disc could be connected to the brow to indicate the required head tilt. Using a mirror to reveal, the patient is rigorously instructed to place the top so that the break is uppermost. With the ocular surface still sterile and the patient supine, the pinnacle and the eye are turned a complete of approximately 45� to one side to place the pars plana injection web site uppermost. The fuel usually is injected temporally except the pars plana epithelium is detached or massive retinal breaks are present in that area, by which case another website is chosen. The needle is directed towards the middle of the vitreous and inserted to a depth of 7 or 8 mm to ensure penetration of the pars plana epithelium and the anterior hyaloid face. The applicable place, with the retinal break uppermost, must be maintained (at least throughout waking hours) for five days. If potential, maintaining the place during sleep is useful, particularly till the retina is reattached. Successful retinal reattachment has been described with positioning for shorter than 5 days, and positioning for 3 days or fewer may usually be enough. Make sure that the needle tip is positioned shallowly inside the vitreous at the time of injection. If fish eggs do occur, the patient is strictly positioned to maintain the bubbles away from retinal breaks. If all retinal breaks are small, this is in all probability not needed, but keep in thoughts that breaks can stretch a little. The bubbles usually coalesce spontaneously within 24 hours, after which the affected person can undertake a place with the retinal break(s) uppermost. Alternatively, the bubbles normally could be triggered to coalesce by flicking the attention with a sterile cotton-tipped applicator or gloved finger. The eye is turned so that sclera without underlying retinal breaks is uppermost, and then this web site is flicked moderately firmly. Since it may not be potential to maintain fish eggs away from superior breaks, this maneuver is very important if massive breaks are present in the superior several clock-hours. Impending macular detachment may also point out this process or point out a face-down position till the bubbles coalesce. Gas Entrapment on the Injection Site After fuel injection, the top is turned to the other side and mobility of the gas is confirmed ophthalmoscopically. At one other website, the gas is reinjected deeper into the vitreous, with 4�5 mm of the needle within the globe. Whether steamrolling is necessary to stop macular detachment is dependent upon several factors: 1. How close the detachment is to the macula (only detachments properly within the arcades usually need steamrolling); 2. If a lot of the fuel is trapped, the affected person is suggested to comply with face-down positioning for 1 day. Thereafter, the patient assumes the desired place with the retinal break uppermost. Waiting for trapped fuel to break away might jeopardize an hooked up macula imminently threatened by detachment. A trapped bubble may be eliminated by passing a 27-gauge needle again through the injection web site. This needle is mounted on a syringe without the plunger, containing a small amount of sterile saline resolution. The entry site is positioned uppermost, and the needle passed vertically into the bubble. Reduction of a bullous detachment overhanging the optic nerve, preventing visualization of the central retinal artery during the procedure. Avoidance of posterior gaping of the tear and subretinal gas within the presence of huge retinal breaks (the excessive example of this being a somersault maneuver performed to unroll the inverted flap of an enormous retinal tear). Second paracentesis and/or ocular compression: if needed to open central retinal artery. Laser to retinal tears: subsequent day or when retina is reattached (in lieu of cryopexy, as two-session procedure), with 360� peripheral laser if desired. Inferior subretinal fluid or loculated pockets of subretinal fluid on uncommon occasion will persist for weeks or months. As a general guideline, the patient is examined on about postoperative days 1 or 2, 5�7, and 14�21 and periodically thereafter, trying particularly for model spanking new retinal breaks. Until it does, the affected person is suggested against air journey as a end result of the decrease atmospheric stress in flight may cause expansion of the gas bubble with a marked increase in intraocular stress. For instance, jarring activities (such as jogging) and rapid head tilting (as with somersaults) are greatest averted. Tornambe17 reviewed the causes of failure and concluded that pseudophakia/aphakia, detachment of >50% of the retina, and multiple retinal breaks adversely affect singleoperation success. An open or absent posterior capsule was associated with an equally decrease single-operation success fee in each teams. Pneumatic retinopexy for the repair of retinal detachments: a comprehensive evaluate (1986�2007). A number of postoperative complications have been noted in the literature, however most of these happen with an incidence of less than 2% (Table 107. The most typical cause of detachment requiring reoperation following pneumatic retinopexy seems to be development of a new retinal break with new rather than persistent retinal detachment. Remarkably, this is less than the 14% figure reported in a study of 171 eyes with retinal breaks without vital retinal detachment, treated with laser photocoagulation or cryopexy but without gasoline injection. However, if fuel does get underneath the retina, the bubble can generally be teased again through the break if the break is larger than the fuel bubble or if the diagnosis is made promptly before gasoline expansion. Under oblique ophthalmoscopic visualization, scleral despair is used to maneuver the bubble to the break and pressure it by way of.
Amoxil 250 mg order with mastercard
Furthermore antibiotic 375mg amoxil 250 mg fast delivery, the rod to cone ratio in rodent retina340 differs from that of the comparatively cone-rich human retina virus 68 symptoms 2014 250 mg amoxil discount with amex. To overcome these problems, animal fashions utilizing bigger eyes, such as the chemically ablated rabbit retina328 and the Abyssinian Rdy cat,341,342 have been employed as properly as normal rabbits,328,343,344 pigs,345,346 and primates. Photoreceptor microaggregates, which are retinal fragments by which tissue integrity is disrupted by mild trituration with cells remaining hooked up to one another in small clusters (<0. Rosette formation prevents the reconstruction of the conventional retinal anatomy and interferes with establishing contacts between graft photoreceptor terminals and host second-order neurons. Sheet preparations protect the organization and polarity of grafted photoreceptors and keep the densely packed arrangement of photoreceptors present in situ and thought to be important for good visual acuity. Studies in neural retinal transplantation have utilized tissue from embryonic, early postnatal, late postnatal, and adult donors in addition to transplantation of homo- and heterotypic neural progenitor cells (stem cells, see below). In one research, makes an attempt to obtain photoreceptor sheets from embryonic retina utilizing vibratome-sectioning resulted in irregular morphology and poor survival. Finally, obtaining embryonic or fetal tissue for transplantation has many logistical and ethical constraints. Adult retinal grafts seem to show normal morphology and organization within the host retina and are related to minimal rosette formation, which could enable for higher restoration of retinal anatomy,328,334,347 particularly if the outer blood�retina barrier remains intact. The methods employed, together with the type of cells used, in these paradigms depend upon the primary derangement that causes photoreceptor cell dying. For example, Schwann cells, derived from peripheral nerves, have been used as autologous grafts to rescue photoreceptors. However, in distinction to Schwann cells, olfactory ensheathing cells had been shown to phagocytose porcine retinal outer segments in an in vitro assay. Transplanted rods may rescue current cones that would be misplaced secondary to rod degeneration. This rescue impact was noticed at a long way from the grafted cells, suggesting the existence of diffusible trophic issue release by the transplant. These findings have been substantiated by in vitro coculture research by which significantly greater numbers of surviving cones had been seen in mouse dystrophic retinas cultured with retinas containing regular rods compared to dystrophic retinas cultured in medium alone or with rod-deprived retinas. In areas where this glial barrier was absent, the transplant and host retinas had been in shut apposition, and their cell processes intermingled indistinguishably. Two weeks later, by which period rd mice lose 97% of rods, the mice had been sacrificed, and the variety of surviving cones in the host retina have been labeled and counted in an unbiased method. Five-week-old unoperated rd mice had been used to determine the baseline price of degeneration over the same 2-week period, and a lack of 30, 000 cones was noted. Only these eyes receiving an outer nuclear layer transplant confirmed a statistically significant higher number of surviving cones (p<. Republished with permission of American Medical Association from Mohand-Said S, Hicks D, Dreyfus H, et al. Similarly, when donor tissue was used in the course of the growth when retina was rich in rod-committed cells, comparable integration into the mature retina was seen after transplantation. The cone-like photoreceptors had been enriched by magneticactivated cell sorting, transplanted into the subretinal area of Nrl(-/-) grownup wild-type mice in addition to cone photoreceptor perform loss 1 mice, and were proven to combine into the host retina, acquire photoreceptor morphology, express conespecific markers, and survive for up to 6 months. Finally, retinal ganglion cell recordings demonstrated photopic responses in retinas with cone cell degeneration, implying restoration of visible function in this mannequin system. Cone integration efficiency seemed to be highest in cone-deficient recipients (Gucy2e-/- mice) compared to Crb1rd8/rd8 mice, which demonstrates that the recipient surroundings can have a profound influence on transplant end result. Furthermore, correct evaluation of visual perform is a complex task, significantly in experimental animals. Simple reflexes, electrophysiologic testing, and visually guided behaviors have been used to evaluate visible perform in laboratory animals. Silverman and coworkers334 reported that visually evoked cortical potentials might be recorded over the retinotopic area that corresponded to the transplant. While the results of these exams are promising, the extent of elicited responses was typically less than that of normal controls. A additional issue is that the validity of a few of these tests as correct measures of visual operate remains controversial. For instance, Kovalevsky and coworkers406 discovered no correlation between the depth of the pupillary gentle reflex and the number of photoreceptor cells present in the host retina. This end result limits the validity of the pupillary gentle reflex as an correct device for evaluating the extent of photoreceptor repopulation or the formation of useful contacts sufficient for the recovery of visible function following retinal transplantation. The hosts had been sacrificed 2 weeks after transplantation, and the eyes were fixed, embedded in agar, and reduce into 60-�m sections. Given that the mind and retina are derived from neuroectoderm and that immature neuronal and progenitor cells are intrinsically able to migrating and differentiating during neural improvement, it will seem that brain-derived neural progenitor cells could doubtlessly differentiate into photoreceptors within the subretinal area. Several groups have examined this possibility408�411 and noted that there was restricted integration of neural progenitor cells into adult host retina,409 but migration of transplanted cells was observed in all layers of a creating immature retina. Similarly, multipotent retinal stem cells isolated from grownup mouse retina had been in a place to efficiently integrate, assume photoreceptor morphology, form synapses with host retinal neurons, and turn out to be useful primarily based on electrophysiologic measurements in rd1 and rd7 mutant mice. These cells develop as neurospheres in culture and give rise to both glial and neural cells. Transplants of M�ller-cellderived stem cells have shown limited integration,432 but treatment of the host retina with chondroitinase (to break down proteoglycans previous to transplantation) resulted in better integration. Typically, tradition of these cells requires the utilization of animal serum or coculture with animal-derived cells. Approval of use of such cells can be problematic due to potential contamination. Similarly, Lamba and coworkers showed that such cells have been able to combine into mouse retina. As noted above, intravitreal bone marrowderived lineage-negative hematopoietic stem cells rescue photoreceptors (primarily cones) in rd1 and rd10 mice. Patients have been followed for as long as forty four months after surgery with no apparent signs of rejection within the absence of immune suppression. Visual enchancment was reported in five transplant recipients however was primarily based solely on subjective testing. Moreover, these sufferers had a point of visual perception preoperatively, which may have been underestimated leading to an apparent increase in visual function after surgical procedure. This affected person additionally showed a 23% improve in mild sensitivity at 5 years compared to microperimetry results at 2 years; the other sufferers showed no improved sensitivity. Patients had been followed for as long as 13 months after surgery with no signs of rejection in the absence of immune suppression. Three patients showed a decline in visible operate, and 3 others confirmed a transient improvement. Ultrastructural and immunocytochemical studies of the eye revealed survival of a minimum of a few of the transplanted cells in the subretinal space with no signs of inflammation. While these studies have established the feasibility and security of retinal transplantation in humans as nicely as the survival of the transplants, further work stays to achieve long-term preservation of visual function. First, immature neural retina is immune privileged tissue,463 and second, the subretinal space is an immune privileged website.
Purchase amoxil 500 mg
Patients with neurofibromatosis have an increased incidence of congenital glaucoma antibiotics for uti child 250 mg amoxil free shipping, which may be secondary to several mechanisms bacteria h pylori symptoms amoxil 500 mg order with mastercard. Multiple iris hamartomas, often known as Lisch nodules, are the most common uveal abnormality of neurofibromatosis type 1. Histopathologically, iris Lisch nodules are hamartomas composed of aggregates of melanocytes on the anterior border layer of the iris. The choroidal findings in sufferers with neurofibromatosis kind 1 embrace unifocal or multifocal choroidal nevus, diffuse plexiform neurofibroma, neurilemoma, and melanoma. Multiple bilateral, choroidal nevi are extremely suggestive of neurofibromatosis sort 1. They might be greatest seen with nearinfrared reflectance imaging or multispectral imaging with lengthy wavelength. Choroidal neurilemoma (schwannoma) is a rare finding and manifests as a circumscribed, amelanotic elevated tumor. There appears to be the next incidence of uveal melanoma in patients with neurofibromatosis. Retinal astrocytic hamartoma is a manifestation of neurofibromatosis, but is more common with tuberous sclerosis complicated. Retinal vasoproliferative tumor can happen with neurofibromatosis, leading to exudative retinopathy and risk for blindness. Dermatologic Features an important cutaneous manifestations of neurofibromatosis embody caf�-au-lait spots (pigmented macules), freckles within the axillary or inguinal area, and urticarial pigmentosa. Caf�-au-lait spots are found in 95% of patients with neurofibromatosis sort 1, but they can be seen in patients with different situations, similar to McCune�Albright syndrome, tuberous sclerosis complex, and Fanconi anemia. They characterize the earliest manifestation of neurofibromatosis kind 1 and can be present in infancy as a very mild hyperpigmented macule that becomes more noticeable over time or with solar exposure. Subcutaneous or cutaneous benign neurofibromas are an essential discovering but are rare in young kids and sometimes seem in older youngsters or later. Plexiform neurofibromas could be invasive and ill-defined, occasionally related to ache. Central Nervous System Features the most important central nervous system function of neurofibromatosis sort 1 is the optic nerve glioma (juvenile pilocytic astrocytoma). Optic nerve glioma can present with apparent features of painless proptosis or subtle features of color or visible acuity abnormalities. Magnetic resonance imaging exhibits enlargement of the optic nerve, often so giant that it develops a fold (kink) within its substance to accommodate the orbit, resulting in down-and-out proptosis. This mass exhibits enhancement on T1-weighted, gadolinium contrast photographs, Phakomatoses 2449 particularly notable within the axial and coronal views. It is essential to differentiate this tumor from optic nerve sheath meningioma because the systemic implications and therapy differ. This is best determined using gadolinium-enhanced, orbital fat suppressed, T1-weighted coronal views. With glioma, the central substance of the nerve enhances whereas with meningioma, the peripheral encircling arachnoid sheath enhances. Glioma is extra usually associated with neurofibromatosis kind 1, whereas meningioma is more related to neurofibromatosis type 2. Sphenoid wing dysplasia, congenital pseudoarthrosis with tibial or forearm bowing, thoracic cage asymmetry with inferior rib prominence, and scoliosis/ kyphosis. A variety of other benign and malignant systemic tumors have been related to neurofibromatosis. Sarcomas can come up from the peripheral nerve sheath, both de novo or from preexisting benign cutaneous nerve sheath tumors. There appears to be an elevated incidence of breast, genitourinary, and gastrointestinal tumors, in addition to cutaneous melanoma. Patients with neurofibromatosis in all probability have a slightly higher incidence of pheochromocytoma. Management the management of neurofibromatosis varies with the location and the extent of the illness. Choroidal melanoma and neurilemoma are sometimes clinically indistinguishable, and have often required plaque radiotherapy, resection, or enucleation. Iris Lisch nodules, congenital hypertrophy of the retinal pigment epithelium, and retinal astrocytic hamartoma are noticed. Retinal vasoproliferative tumors often require cryotherapy, laser photocoagulation, photodynamic therapy, or plaque radiotherapy to control exudative findings. The incidence of neurofibromatosis sort 2 is 1 in 25,000 stay births and has nearly 100% penetrance by 60 years of age. When mutated, decreased perform of merlin results in the uncontrolled improvement of tumors, significantly within the central nervous system. The juvenile posterior subcapsular cataract (<50 years) is a criterion for analysis of this situation. Other lens opacity within the capsular or cortical region of younger sufferers are believed related to neurofibromatosis kind 2. Of those with severe medical options of neurofibromatosis type 2, 80% display epiretinal membranes. Early age at symptom onset and the presence of intracranial meningioma at analysis are two signs of higher danger for disease severity and mortality. In an analysis of Dermatologic Features the cutaneous options of neurofibromatosis kind 2 are slightly totally different than those in sort 1. Neurofibromatosis type 2 displays skin plaques, represented by well-circumscribed, roughened areas lower than 2 cm and sometimes with slight hyperpigmentation and hypertrichosis. Other Features Sensory motor polyneuropathy may be discovered, significantly in these with schwannomas. Central Nervous System Features Neurofibromatosis sort 2 is also called central nervous system neurofibromatosis because of the importance of those associated tumors. The central nervous system tumors represent nearly all of findings in neurofibromatosis type 2 and vary with the dimensions and extent of the related tumors. Acoustic neuromas (vestibular schwannomas) are the most typical and well-recognized function. Patients present with signs of tinnitus, gradual listening to loss, and later development produces brainstem compression, hydrocephalus, and facial palsy. Surgical resection of symptomatic neurologic tumors is carried out, but radiotherapy or chemotherapy can be used, particularly for ependymomas. Erlotinib and lapatinib (epidermal progress issue inhibitors) for unresectable progressive schwannomas is beneath trial. These embrace choroidal hemangioma, facial nevus flammeus (port wine stain), and brain hemangioma with intracranial calcification.
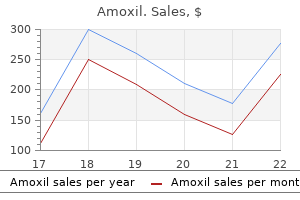
| Comparative prices of Amoxil |
| # | Retailer | Average price |
| 1 | O'Reilly Automotive | 884 |
| 2 | DineEquity | 819 |
| 3 | Sherwin-Williams | 861 |
| 4 | J.C. Penney | 541 |
| 5 | Giant Eagle | 224 |
| 6 | Walgreen | 782 |
| 7 | Starbucks | 339 |
| 8 | Tractor Supply Co. | 809 |
| 9 | Neiman Marcus | 551 |
Generic amoxil 250 mg on-line
Delayed regression antibiotics for lower uti amoxil 250 mg amex, observed in some irradiated tumors antibiotics for uti nausea amoxil 500 mg with mastercard, is probably as a result of extended intermitotic phases of melanoma cells. This protracted pattern of tumor regression has been supported by histologic research of tumors enucleated at varying instances after proton therapy, which confirmed a larger decline of mitotic figures with longer periods between irradiation and enucleation. In eyes with tumors positioned farther than 3 mm from these constructions, tumor destruction often occurs without functionally significant radiation vasculopathy. Risk factors for vision loss included dose to the macula, tumor height, poorer baseline imaginative and prescient, and a historical past of diabetes. For instance, in our collection of proton-irradiated massive tumors (height 10 mm (or eight mm if optic nerve involved) or top 2 mm and diameter >16 mm), close to half (46. Despite having massive tumors, preirradiation visible acuity was 20/40 or higher in over one-third of those patients. By 5 years after therapy, nevertheless, nearly all of sufferers had experienced extreme visible decline (84% had imaginative and prescient worse than 20/200 and 69% had imaginative and prescient worse than counting fingers). Visual prognosis after proton irradiation for sufferers with peripapillary and parapapillary tumors is poor, with a 5-year fee of imaginative and prescient loss to worse than 20/200 of 80%. Patients with macular tumors also have an elevated danger of visible loss, with a minority of patients (35. In patients with large tumors, intratumor hemorrhage might sometimes happen as a end result of surgical manipulation. Corneal epitheliopathy has developed in a small number of instances with large ciliochoroidal melanomas and normally responds to synthetic tears. In macular and paramacular melanomas (<3 mm from the fovea), radiation maculopathy and papillopathy may develop resulting in imaginative and prescient loss. By 5 years after proton therapy, radiation papillopathy developed in 81% of circumstances by which the melanoma abutted the optic nerve and in 67% of cases in which the melanoma was zero. Of those who developed papillopathy, 42% retained vision of counting fingers or higher and 31% (n=13) experienced recovery of visible acuity after an initial loss. Significant cataracts could develop in sufferers with ciliary body involvement or in instances of highly elevated choroidal melanomas by which the lens receives substantial irradiation. Rates had been dependent upon the dose to the lens; at 5 years post-therapy, 53% developed cataract when >50% of the lens was irradiated compared with 19% when <10% of the lens was irradiated. For eyes with reasonable visual potential, cataract extraction with intraocular lens implantation may be carried out. Approximately 50% of sufferers present process cataract extraction after proton beam irradiation for choroidal melanoma had visual acuity of 20/200 or higher after surgical procedure. In an effort to cut back the ocular morbidity related to proton therapy, significantly when tumors are situated near critical constructions, a randomized, double-blind dose discount trial23 was accomplished. Patients eligible for the trial have been at excessive threat of radiation papillopathy and maculopathy as a outcome of their tumors had been positioned near the optic nerve or macula. This degree of dose reduction (28%) may be inadequate to produce appreciable improvement in useful outcomes, however additional reductions may compromise tumor management. Radiation of the tumor with a decrease dose grew to become standard at our center for select sufferers with small or medium tumors situated near the optic nerve or fovea in May 2004. Further study to identify possible useful results of a dose discount, general and in particular subgroups of patients, is presently underway on this bigger cohort of sufferers. Recurrence Local recurrence after charged-particle irradiation is noticed in 2�5%24�26,forty three of sufferers. In one study34 of 2069 consecutive patients handled with proton beam irradiation, forty five tumors (2. Only 23 had been marginal recurrences; in the case of anterior tumors involving the ciliary physique, marginal recurrences may arise because the pigmented margins of the tumor may be difficult to distinguish from surrounding stroma. Six recurrences had been ring melanomas, eight concerned extrascleral extension of the tumors, and 9 confirmed vertical development of the tumors. An additional 15 eyes were enucleated at other facilities because tumor growth was suspected. Similar management rates have been reported in another large series of sufferers (n=2435) handled in Lausanne, Switzerland. Proton irradiation has additionally been used successfully to treat patients with tumor recurrences that were initially treated by different means. Proton irradiation could additionally be a better choice of treatment for posteriorly located tumors. MetastasisandSurvival Annual charges of melanoma-related mortality are highest 3�6 years after irradiation, but patients proceed to be in danger a few years after prognosis. A latest study compared sufferers who had been identified with metastatic uveal melanoma after proton irradiation incidentally or by routine surveillance to those who have been identified after developing signs. Few remissions have been realized with chemoembolization of the liver and immunotherapy with interleukin-2, alone or in combination with other chemotherapeutics, and toxicity is excessive. Results of nonrandomized research evaluating survival charges for patients with uveal melanoma after remedy with proton beam irradiation71 and other types of radiotherapy72 with survival charges after enucleation counsel that remedy choice has little effect on survival. Results from the Collaborative Ocular Melanoma Study confirmed no variations in 5-year rates of death as a end result of histopathologically confirmed metastatic melanoma between patients randomized to bear Enucleation the probability of retaining the eye 2 years after proton irradiation is 95%, and the probability is 90% after 5 years. The main threat factors for enucleation are tumor top,34,56 proximity of the tumor to important buildings (macula, fovea,fifty six optic nerve), tumor diameter, tumor pigmentation, and tumor shape. The dose distributions are particularly advantageous for the remedy of large tumors and tumors situated near the optic disc or fovea, with many patients maintaining visible perform in the handled eye. Nevertheless, there may be important ocular morbidity related to remedy of such instances. Outcomes after remedy of radiation complications with systemic corticosteroids and anticoagulation have been disappointing,seventy three,74 however preliminary reviews of intravitreal triamcinolone,75 bevacizumab,76-78 and combination remedy with these compounds79 suggest some efficacy for radiation maculopathy and papillopathy. Encouraging results have been reported for prophylactic bevacizumab to scale back rubeosis after proton radiation. Another unresolved concern is the optimum fractionation scheme and dose for therapy. Fractionation of the dose is essential in optimizing the relative responses of tumor and normal tissue to irradiation. However, the optimal radiation dose that may control a melanoma with minimum ocular morbidity is unknown. Current results suggest that main therapy alternative has little overall influence on survival in sufferers with uveal melanoma. It is most likely going that micrometastasis occurs before any type of ocular treatment has been initiated. Therefore, efforts towards the event of efficient adjuvant therapies should proceed. Local tumor management, visible acuity, and survival after hypofractionated stereotactic photon radiotherapy of choroidal melanoma in 212 sufferers treated between 1997 and 2007. Radiogenic unwanted effects after hypofractionated stereotactic photon radiotherapy of choroidal melanoma in 212 patients handled between 1997 and 2007. Preliminary outcomes of proton beam irradiation of macular and paramacular melanomas. Exploratory research of proton radiation therapy using large field methods and fractionated dose schedules. Outcomes of therapy with stereotactic radiosurgery or proton beam therapy for choroidal melanoma.
Cheap amoxil 250 mg otc
If retinal holes are detected under proliferating tissue or created throughout preparation antibiotics for uti nz amoxil 250 mg cheap fast delivery, the encompassing tissue must be excised with out residual traction antibiotics before root canal amoxil 250 mg without prescription. Also right here, some perfluorocarbon may be useful to flatten out a localized retinal detachment and facilitate enough laser therapy of the holes. As already mentioned above, careful panretinal laser therapy is carried out once the retina is cleaned. The tamponade of alternative may be both a longeracting gasoline tamponade or silicone oil. The use of some perfluorocarbon to prevent bleeding into the foveal area can be useful if a bridging membrane has been eliminated, but additional dissection must be done within the midperipheral retina. Core vitrectomy is performed with lesser suction than usual, and the tissue is carefully inspected before slicing. Once a clear overview of the retinal scenario is created, dissection of tissue is started usually in an space distant from the indifferent retina. Perfluorocarbon can be used to stabilize the posterior retina, whereas further tissue removing in the periphery is carried out. However, if an atrophic retinal detachment is current, the use of perfluorocarbon can be dangerous because the retina is inelastic and shortened. A primarily small retinal hole can turn into a large retinal hole, and perfluorocarbon may glide within the subretinal area. A comparable situation can occur when silicone oil tamponade is used too early and the retina is still under traction. Careful inspection of the periphery under indentation is needed, and anteriorly dislocated retina is both free of fibrotic tissue or reduce. Retinectomies and retinotomies ought to be used only in selected circumstances and carried out as a last resort (see additionally Chapter 112, Retinotomies and retinectomies). Usually peripheral retinectomies are wanted in eyes where reoperations become necessary and severe anterior hyaloid fibrovascular proliferation has developed. Before the retina is reduce, diathermy is utilized to the anterior and posterior margin of the retina and the vessels to be excised. The extension of the retinotomy ought to reach normal retinal space across the area of traction. If not already indifferent, a shallow detachment must be created so as to reduce without traumatizing the choroid or creating hemorrhage. It is obligatory in diabetic vitrectomy to release all tractions around retinal holes before tamponades can be used. The anterior part of the retina is also trimmed and cauterized in retinectomies to keep away from secondary fibrosis of residual anterior retina and traction on surrounding tissue and/or the ciliary physique. Smaller posterior retinotomies also can turn into necessary if persistent traction around an old tear exists. Silicone oil is the tamponade of selection for diabetic eyes requiring retinectomies. Eyes requiring retinectomies have a poorer consequence and visible prognosis than those not requiring them. It is normally performed in reoperations or as a primary surgery in youthful diabetic sufferers the place large exercise and fibrovascular proliferation and detachment exist, however visible acuity remains to be helpful. In major procedures, the retina is usually more elastic and an extra encircling band would possibly make a big retinectomy pointless. The conjunctiva is dissected over 360� at 1�2 mm distance from the limbus, and Tenon capsule peritomy performed. Four-0 sutures are positioned under every rectus muscle and 4 5-0 nylon mattress sutures prepared in each quadrant to safe the band. The anterior suture is placed 2�4 mm behind the insertion of the rectus muscular tissues; the posterior suture depends on the dimensions of the band. For a 4-mm band, no much less than a 6-mm distance between sutures has to be chosen to find a way to create indentation. When the silicone band is placed underneath the muscle tissue and the sutures (or tunnels), sutures are fastened and the ends of the band secured with a variety of selections. Certainly fixation of the cerclage could be postponed until after vitrectomy, but this makes a change from internal surgery to external surgical procedure needed. In eyes the place lens surgery is planned, an inferior sclerotomy is positioned to permit some liquefied vitreous to escape. If the anterior chamber is deep enough to allow cataract surgery, a small limbal incision is carried out and the anterior chamber filled with viscoelastic. A permanent or transient 10-0 nylon suture to seal the cataract wound is advisable in complex diabetic vitrectomy, where adjustments in intraocular stress could be anticipated throughout and after surgical procedure. Photocoagulation Panretinal photocoagulation with an endophotocoagulation probe is at all times performed throughout diabetic vitrectomy to achieve regression of neovascularizations and to create adhesions around retinal breaks, retinotomies, and retinectomies. The adequate coagulation impact requires apposition of the retina to the retinal pigment epithelium, which eventually requires using intraoperative internal tamponades, as gas or perfluorocarbon liquids. The angle of the instrument in relation to the retinal airplane may also affect intensity of the coagulates. Whitish laser results ought to be seen; nevertheless, hard hyperintense remedy must be avoided. As a short-term intraoperative instrument, heavy perfluorocarbon liquid is mostly used. It is helpful to reattach the retina, permitting panretinal photocoagulation or membrane dissection. Perfluorocarbon have to be utterly eliminated earlier than the top of surgery due to retinotoxic results. For a fluid�air change, infusion is turned off and air is provided through the infusion port with a continuous air pump. A silicone-tipped fluid needle or cannula is then used to aspirate the fluid from the vitreous cavity. If subretinal fluid is current, it can be aspirated by way of a preexisting or iatrogenic retinal break. Gases are preferred tamponades for superior or posterior pathologies or in patients the place positioning is possible. If nitrous oxide is used generally anesthesia, it must be discontinued 20 minutes before gasoline injection to stop excessive nitrogen in the fuel bubble, resulting in an undesirably small postoperative fuel bubble. In aphakic eyes, an inferior ("Ando"-) iridectomy should be created to forestall silicone oil from getting into the anterior chamber. If potential, silicone oils ought to be eliminated after a number of (3�6) months to keep away from late silicone-related issues, as cataract, secondary glaucoma, keratopathy, or optic disc atrophy. During closure of the superior sclerotomies, the infusion maintains a steady intraocular strain; if self-sealing incisions had been used, the intraocular strain should be slightly lowered before elimination of the cannulas. In 20-gauge vitrectomy, sclerotomies are sutured rigorously with partial-thickness 7-0 or 8-0 Vicryl sutures. In 25- or 23-gauge transconjunctival small incision vitrectomy, wounds can stay unsutured.
Generic amoxil 250 mg amex
Monosomy three virus your current security settings amoxil 500 mg discount mastercard, tumor location bacteria arrangement purchase amoxil 500 mg overnight delivery, and tumor diameter had been the most important predictors of poor prognosis. Furthermore, histologic subtype, age, sex, extrascleral growth and tumor thickness had no predictive value. The tumors clustered into two groups that correlated strongly with metastatic danger. A "Class 1" tumor designation indicated a low-risk for metastasis; a "Class 2" designation indicated a excessive risk for metastasis. Prognosticating the danger of developing metastatic uveal melanoma has traditionally been primarily based on medical and histopathologic characteristics of the primary tumor, as mentioned beforehand. However, as nearly all of uveal melanomas are now being treated with globe-sparing surgery, evaluation of molecular and cytogenetic info from uveal melanoma fine-needle aspiration biopsy has advanced and is changing into more and more frequent. These associations could also be either markers of aggressive tumors without direct contribution to the metastatic cascade or they may point out direct participation in tumor development to metastasis. High microvascular density could assist to predict survival after detection of hepatic metastases. The presence of networks of three or more contiguous closed vascular loops was highly predictive of melanoma-related and all-cause mortality. Principal part evaluation of vascular patterns from this cohort of patients128 identified three combinations of patterns, two of which � disordered growth and emergence of quickly growing subclones � had been predictive of melanoma mortality. Extrascleral Extension Another issue proven in plenty of research to improve the chance of tumor-related demise after enucleation is extrascleral extension of the tumor. The 5-year survival rate was 26% in patients with orbital extension and 78% in those with out extension. The relationship between the likelihood of not dying of melanoma and the presence of extrascleral extension was evaluated in another group of patients using new statistical strategies in 1983, including Kaplan�Meier survival curves and Cox proportional hazards models. A recent report by Klufas and colleagues indicated that nonmelanoma tumor tissue may also give Class 1 and Class 2 test outcomes, regardless of there being no melanoma cell sort present. Although the specific chromosomal abnormalities, specifically monosomy three, may be essential in predicting most cancers prognosis with respect to metastasis, the utilization of molecular markers and/or mutations of biologic relevance have yet to be found. In the long run, tumor tissue could additionally be screened for these markers, which could assist tailor therapies for uveal melanoma metastasis when such treatments exist. Currently, regardless of therapy with present chemotherapeutic regimens, patients with metastases from uveal melanoma usually die inside 2�14 months after the prognosis of disseminated disease and the prognosis has not considerably improved over the decades. We want a better understanding of the biologic mechanisms contributing to growth and progression of metastatic uveal melanoma. Despite the continuous emergence of latest eye-conserving therapies, radiation is the superior treatment of choice to reduce the serious morbidity of local therapy failure. A higher understanding of the molecular events leading to metastasis, together with mobile differentiation, adhesiveness, and vascular biology, could assist in the development of recent systemic therapies. With the growing use of fine-needle aspiration biopsy to get hold of molecular info for metastatic prognosis, a chance for finding out primary tumor biology exists which might lead to a greater understanding of uveal melanoma metastasis and prognosis. Intraoperative echographic localization of iodine-125 episcleral plaque for brachytherapy of choroidal melanoma. Local control and visual acuity following remedy of medium-sized ocular melanoma utilizing a contact eye plaque: a single surgeon experience. This has been debated with skeptics citing the likelihood of lead-time bias for the event of metastasis when smaller tumors are treated. Damato and colleagues reported that sufferers who had been younger at remedy had smaller tumors and had a decrease price of metastatic consequence. Results based on outcomes in over 3000 patients over a couple of 20-year interval recommend that remedy may stop tumor development, dedifferentiation, and metastatic illness in some patients, particularly these with smaller tumors. With earlier detection and enchancment within the ability to diagnose, biopsy, and deal with small choroidal melanomas, evaluation of metastatic end result might be crucial. It may be possible to not solely achieve local tumor control in patients with small choroidal melanoma, but additionally influence metastasis in this subset of patients. For sufferers managed by initial statement, the decision to deal with and the timing of therapy depend upon clinical judgment. Conservation of eyes with choroidal melanoma by a multimodality method to therapy: an audit of 1632 sufferers. Transscleral resection versus iodine brachytherapy for choroidal malignant melanomas 6 millimeters or more in thickness: a matched case�control examine. Long-term surgical end result of posterior choroidal melanoma treated by endoresection. Tumor doubling occasions in metastatic malignant melanoma of the uvea: tumor development earlier than and after treatment. Standardized data assortment and coding in eye disease epidemiology: the uveal melanoma information system. Comparison of survival rates for patients with uveal melanoma after remedy with proton beam irradiation or enucleation. A prognostic factor study of disease-free interval and survival following enucleation for uveal melanoma. Uveal melanomas close to the optic disc or fovea: visual results after proton beam irradiation. A 17-year retrospective research of institutional outcomes for eye plaque brachytherapy of uveal melanoma utilizing (125)I, (103)Pd, and (131)Cs and historical perspective. Comparison of episcleral plaque and proton beam radiation remedy for the remedy of choroidal melanoma. Transscleral local resection versus iodine brachytherapy for uveal melanomas that are giant because of tumour top. Proton beam radiotherapy of uveal melanoma: Italian patients treated in Nice, France. Long-term danger of local failure after proton therapy for choroidal/ciliary physique melanoma. Attenuation of iodine-125 radiation with vitreous substitutes within the treatment of uveal melanoma. The effects of intraocular silicone oil placement previous to iodine-125 brachytherapy for uveal melanoma: a medical case sequence. Iodine-125 brachytherapy with vitrectomy and silicone oil within the remedy of uveal melanoma: 1-to-1 matched case-control sequence. Extrascleral extension of a choroidal melanoma after argon photocoagulation and transpupillary thermotherapy. Photodynamic remedy with verteporfin in subfoveal choroidal melanoma (a controlled case). Primary transpupillary thermotherapy for small choroidal melanoma in 256 consecutive cases: outcomes and limitations. Long-term outcomes of major transpupillary thermal remedy for the therapy of choroidal malignant melanoma.
Buy amoxil 250 mg with visa
These observations and workup are often hampered by poor visualization ensuing from posterior synechiae virus 58 symptoms amoxil 500 mg buy generic line, cataract virus 404 error amoxil 250 mg discount, vitreous haze, or cellular infiltration. If visualization of the vitreoretinal interface becomes difficult and therapy with intravitreal steroids is envisaged, triamcinolone will improve the ultrasound signal and facilitate visualization of posterior structures. Ciliary physique detachments may develop because of uveitis, causing or predisposing to hypotony. In postherpetic detachments, tears are sometimes positioned on the margin of the atrophic scar or at the insertion of the posterior hyaloid onto the retinal floor. Vitreous condensation and contraction onto the posterior iris surface has also led to traction and detachment on the ciliary processes. The more in depth the area of gliosis, the extra probable is the development of a detachment. It is essential to adequately and aggressively manage the inflammatory part with a mix of systemic and local remedy. The selection will depend upon the nature of inflammation and previous response to remedy. If the iris requires manipulation throughout surgical procedure, prostaglandin inhibitors must be added topically in addition to systemically starting the day previous to surgery. This is commonly accomplished in uveitis patients present process cataract surgical procedure as it could significantly scale back postoperative anterior segment inflammation. The use of a long-acting (or gradual release) steroid preparation will scale back the severity of any recurrence growing within the postoperative interval. In general, higher surgical success is obtained when a extra aggressive strategy is taken. Lens extraction must be considered, even within the presence of a transparent lens, in all instances requiring vitreous base shaving or when a major postoperative fibrinous response is anticipated. It may be very difficult to achieve an enough ablation of anterior vitreous over 360� with out elimination of the lens. Anterior displacement of the lens by draining the anterior chamber is regularly not adequate. In the absence of energetic irritation, most instances respond as if they have been uncomplicated retinal detachments, and thus the benefit outweighs the surgical threat. As in every case of intraocular surgery on uveitis patients, outcomes are finest if inflammation is absent. The vitrectomy is normally initiated after removing of the crystalline lens and its replacement with an intraocular lens. As indicated by the authors, this strategy is supposed to drain persistent subretinal fluid in patients with quiescent inflammation. Delaying intraocular surgical procedure in these patients is a valid strategy, since successful surgical reattachment, as a quantity of research have suggested, is usually associated with a point of central lack of imaginative and prescient, presumably related to microangiopathy, optic neuropathy, or silicone-oil-related toxicity. When preexisting vitreous separation is present, the posterior hyaloid is identified and resected as much as the posterior margin of the vitreous base. If it may be mechanically engaged and simply elevated from the retina, this is carried out to create a posterior vitreous separation. An try should be made to resect the vitreous as close to the surface of the retina as possible, without inducing a vitreous detachment. Many surgeons advocate demarcating the atrophic areas with laser, in addition to those areas that are prone to harbor retinal breaks. The choice will depend on the configuration of the detachment and the likelihood of recurrent exercise. Postoperative follow-up is aimed toward identifying proof of silicone oil toxicity, reactivation of the viral infection, and to detect recurrent retinal detachment. Typically, the recurrent retinal detachment is shallow and positioned inferiorly, where the silicone bubble may not be entirely in contact with the retina. Peeling is facilitated by utilizing perfluorocarbon, which acts as a "third" harm, providing posterior stabilization to the membranes being peeled. Once the retina is totally reattached beneath perfluorocarbon, the perimeters of the tears are treated by photocoagulation. Cryotherapy should be avoided, because it enhances breakdown of the blood�ocular barrier and might increase postoperative inflammation. It can be thought to restrict the accumulation of proinflammatory cytokines within the vitreous cavity. In all cases a scleral buckle was used to present peripheral help in the area of drainage. If the macula is threatened or detached in a watch with beforehand good imaginative and prescient, then reoperation could also be warranted. Often, drainage of subretinal fluid combined with injection of extra silicone with further photocoagulation is the remedy of selection. If visualization is poor, the oil have to be removed and the retina reattached, as described above, before the oil is reinjected. Lensectomy may be essential, preferably with the implantation of an intraocular lens, maintaining the posterior capsule. Later capsular opacification is frequent, nonetheless, and one should contemplate main capsulotomy in selected instances. Looking on the nerve to keep away from a pulsatile perfusion at the onset of surgical procedure, and periodically throughout surgery, can avoid additional loss of vision from prolonged retina anoxia. A lens extraction is required in practically all circumstances to expose the complete extent of the vitreous base so that every one condensed vitreous and vitreous traction can be eradicated. Posterior epiretinal membranes overlying healthy retina are recognized and eliminated with choose and forceps. Once the posterior healthy retina is freed from membranes, perfluorocarbon is used to tamponade this retina out to the edge of atrophic retina. As that is nonfunctional retinal tissue, it has no physiologic function and may finest be eliminated. Larger vessels, even though these are attenuated, ought to be treated with diathermy as they could bleed. This could result in a 360� retinotomy leaving a reasonably central area of viable, wholesome retina. Once the vitreous, preretinal membranes, and indifferent atrophic retina have been removed, remaining retinal breaks are recognized and marked with endodiathermy. Under perfluorocarbon the sting between healthy and any remaining atrophic retina, in addition to the free edge that was created earlier, are treated by endophotocoagulation, putting several rows of laser along the edge of wholesome retina. If peripheral support is critical, particularly inferiorly, an encircling band or an entire scleral buckle could be positioned. The oil ought to be ideally removed in 3�6 months to keep away from long-term complications related to its presence. Removal ought to be thought-about provided that the danger of redetachment is believed to be minimal. In addition in these situations, the surgical procedure ought to be carried out as a lot as potential with a low intraocular strain, because the circulation by way of the optic nerve may be occluded at even normal infusion pressures. Reducing these molecules can improve the prognosis and implies a concerted local and systemic effort to reduce intraocular inflammation. It is finest achieved as a group effort between the vitreoretinal surgeon and the uveitis specialist.
Amoxil 500 mg on-line
If the palpebral aperture is deemed too slim antibiotic 3 pills generic amoxil 500 mg without a prescription, a lateral canthotomy may be carried out antibiotic resistance legislation amoxil 500 mg discount without a prescription. Recession of the peritomy edge leaves naked sclera and makes subsequent reoperation tough. A second cut is commonly wanted to lengthen the incision via the Tenon capsule right down to the sclera. The spring scissors can simply be utilized in both hand and the orientation diversified because the incision progresses. A light spreading action of the scissors underneath the conjunctiva breaks the weak trabecular adhesions to the episcleral tissue. Slinging Rectus Muscles Between two and four rectus muscular tissues are slung relying on the planned dimension of the buckle. A closed pair of blunt scissors is pushed by way of the intermuscular septum between two recti. If the muscle is inadvertently break up, a second hook can be handed from the alternative side of the muscle. There are varied ways of achieving this involving reverse passage of the suture under the muscle (to avoid engaging the tip in the sclera). Alternatively, a modified muscle hook with a threading eyelet at its tip can be utilized. Suturing and even cryotherapy or indentation at these sites can be perilous, so their early identification is important. A slicing action with the scissors is more effective than a spreading motion in breaking these. Care have to be taken to keep away from delaminating into the sclera or buttonholing conjunctiva. The muscle hooks are placed around the muscular tissues over the explants earlier than these are removed. The sclera is often very skinny within the bed of longstanding buckles, particularly encircling components. Particular care should be taken when dissecting the capsule from the very skinny sclera beneath the rectus muscles. Examination Under Anesthesia and Break Localization A careful indented examination under anesthesia of the whole peripheral retina is now carried out to affirm the location of the retinal breaks. Some surgeons advocate microscopic visualization using endoillumination (such as a chandelier inserted through the pars plana) in combination with an indirect viewing system such as the Biom. This important step is carried out whereas the cornea is obvious and permits planning of the rest of the operation. The sclera is indented under oblique ophthalmoscopic indentation using a fantastic (but not sharp) tipped instrument such as a Gass scleral indenter. The resulting transient scleral thinning produces a focal area of scleral translucency, and the underlying choroid shows by way of. If a marker pen is used, the sclera is dried both earlier than and after the application to stop the dye spreading. The development of corneal opacity greatly complicates surgical procedure, particularly if it develops in the early levels of the procedure. This ought to be prevented by using preservative-free drops for preoperative pupil dilatation and avoiding the corneal epithelium desiccation by periodic irrigation with saline or use of a coating of dispersive viscoelastic. If corneal epithelial edema develops, the view could additionally be transiently improved by rolling a humid cotton bud over the cornea accompanied by slight downward strain on the globe. Whenbreaksarehighlyelevated, they appear extra posterior than they really are because of parallax. Retinopexy the indent from the explant closes retinal breaks, however retinopexy is required to produce a permanent bond between the retina and the retinal pigment epithelium that may persist even when the indent disappears. Cryotherapy the technique of cryotherapy is described intimately in Chapter one hundred ten (Prevention of retinal detachment). The purpose is to produce freezing of healthy retina surrounding all the retinal breaks. When the indent from the tip of the cryoprobe is seen beneath a retinal break, the cryoprobe is activated. The break is seen as a darker area throughout the freeze, and that is helpful in confirming that the entire break has been treated. Some components (the insulating impact of an intervening rectus muscle, the warmth sink impact of the choroidal circulation) impede the event of a visible reaction on the retina. Others (reduced choroidal blood flow in high myopia, the insulating impact of intraocular gas) hasten the development of retinal freezing. In the presence of shallow subretinal fluid, the indentation of the tip of the cryoprobe approximates the pigment epithelium to the retina and both freeze virtually concurrently. This is a very essential query given the concern about potential adverse results of excessive cryotherapy on different tissues. The ensuing chorioretinal adhesion was weaker than when the freeze was allowed to prolong to the retina. A additional advantage of freezing the retina, nonetheless, is that the "lighting up" of the retinal breaks is a helpful affirmation that every one the perimeters of the break have been treated. In the presence of bullous subretinal fluid, it might be impossible to approximate the retina to the retinal pigment epithelium. In this situation, subretinal fluid drainage is probably safer than very heavy cryotherapy, which can trigger severe postoperative vitritis. The tip of the cryoprobe have to be allowed to thaw fully earlier than tried withdrawal, otherwise choroidal hemorrhage and even scleral avulsion may happen. This cognitive downside may be prevented by encouraging trainees to deliberately indent posteriorly (without actually activating the cryoprobe! Beginners discover cryotherapy on anterior breaks challenging as a result of the cryoprobe tends to slip over the surface of the eye. Alternatively, the cryoprobe is deliberately placed anterior to the break and the globe rotated using the tip of the probe. The pressure of the probe is then barely launched while the indent from the probe is considered utilizing indirect ophthalmoscopy. As the globe returns slowly to the first position, the tip indentation is seen to move. When the indentation of the tip is under the break, a really small increase within the strain applied stabilizes the globe and the cryoprobe is activated. The delivery strategy of transscleral diode laser makes use of a probe that indents the sclera underneath indirect ophthalmoscopic visualization. The endpoint of therapy can be troublesome to titrate, particularly in blonde fundi, and overtreatment with choroidal hemorrhage and scleral thinning might happen during the studying curve. Photocoagulation on the buckle is uncomfortable and requires using regional anesthesia.